{"title":"抗利尿激素在心力衰竭中的拮抗作用:血流动力学研究和主要临床试验的综述。","authors":"Jonathan Urbach, Steven R Goldsmith","doi":"10.1177/1753944720977741","DOIUrl":null,"url":null,"abstract":"For decades, plasma arginine vasopressin (AVP) levels have been known to be elevated in patients with congestive heart failure (HF). Excessive AVP signaling at either or both the V1a and V2 receptors could contribute to the pathophysiology of HF by several mechanisms. V1a activation could cause vasoconstriction and/or direct myocardial hypertrophy as intracellular signaling pathways are closely related to those for angiotensin II. V2 activation could cause fluid retention and hyponatremia. A hemodynamic study with the pure V2 antagonist tolvaptan (TV) showed minimal hemodynamic effects. Compared with furosemide in another study, the renal and neurohormonal effects of TV were favorable. Several clinical trials with TV as adjunctive therapy in acute HF have shown beneficial effects on fluid balance and dyspnea, with no worsening of renal function or neurohormonal stimulation. Two smaller studies, one in acute and one in chronic HF, have shown comparable clinical and more favorable renal and neurohormonal effects of TV compared with loop diuretics. However, long-term treatment with TV did not alter outcomes in acute HF. No data are available other than single-dose studies of an intravenous pure V1a antagonist, which showed a vasodilating effect if plasma AVP levels were elevated. One hemodynamic study and one short-duration clinical trial with the balanced intravenous V1a/V2 antagonist conivaptan (CV) showed hemodynamic and clinical effects largely similar to those with TV in similar studies. A new orally effective balanced V1/V2 antagonist (pecavaptan) is currently undergoing phase II study as both adjunctive and alternative therapy during and after hospitalization for acute HF. The purpose of this review is to summarize what we have learned from the clinical experience with TV and CV, and to suggest implications of these findings for future work with newer agents.","PeriodicalId":23035,"journal":{"name":"Therapeutic Advances in Cardiovascular Disease","volume":"15 ","pages":"1753944720977741"},"PeriodicalIF":2.2000,"publicationDate":"2021-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/1753944720977741","citationCount":"14","resultStr":"{\"title\":\"Vasopressin antagonism in heart failure: a review of the hemodynamic studies and major clinical trials.\",\"authors\":\"Jonathan Urbach, Steven R Goldsmith\",\"doi\":\"10.1177/1753944720977741\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"For decades, plasma arginine vasopressin (AVP) levels have been known to be elevated in patients with congestive heart failure (HF). Excessive AVP signaling at either or both the V1a and V2 receptors could contribute to the pathophysiology of HF by several mechanisms. V1a activation could cause vasoconstriction and/or direct myocardial hypertrophy as intracellular signaling pathways are closely related to those for angiotensin II. V2 activation could cause fluid retention and hyponatremia. A hemodynamic study with the pure V2 antagonist tolvaptan (TV) showed minimal hemodynamic effects. Compared with furosemide in another study, the renal and neurohormonal effects of TV were favorable. Several clinical trials with TV as adjunctive therapy in acute HF have shown beneficial effects on fluid balance and dyspnea, with no worsening of renal function or neurohormonal stimulation. Two smaller studies, one in acute and one in chronic HF, have shown comparable clinical and more favorable renal and neurohormonal effects of TV compared with loop diuretics. However, long-term treatment with TV did not alter outcomes in acute HF. No data are available other than single-dose studies of an intravenous pure V1a antagonist, which showed a vasodilating effect if plasma AVP levels were elevated. One hemodynamic study and one short-duration clinical trial with the balanced intravenous V1a/V2 antagonist conivaptan (CV) showed hemodynamic and clinical effects largely similar to those with TV in similar studies. A new orally effective balanced V1/V2 antagonist (pecavaptan) is currently undergoing phase II study as both adjunctive and alternative therapy during and after hospitalization for acute HF. The purpose of this review is to summarize what we have learned from the clinical experience with TV and CV, and to suggest implications of these findings for future work with newer agents.\",\"PeriodicalId\":23035,\"journal\":{\"name\":\"Therapeutic Advances in Cardiovascular Disease\",\"volume\":\"15 \",\"pages\":\"1753944720977741\"},\"PeriodicalIF\":2.2000,\"publicationDate\":\"2021-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1177/1753944720977741\",\"citationCount\":\"14\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Cardiovascular Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/1753944720977741\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/1753944720977741","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Vasopressin antagonism in heart failure: a review of the hemodynamic studies and major clinical trials.
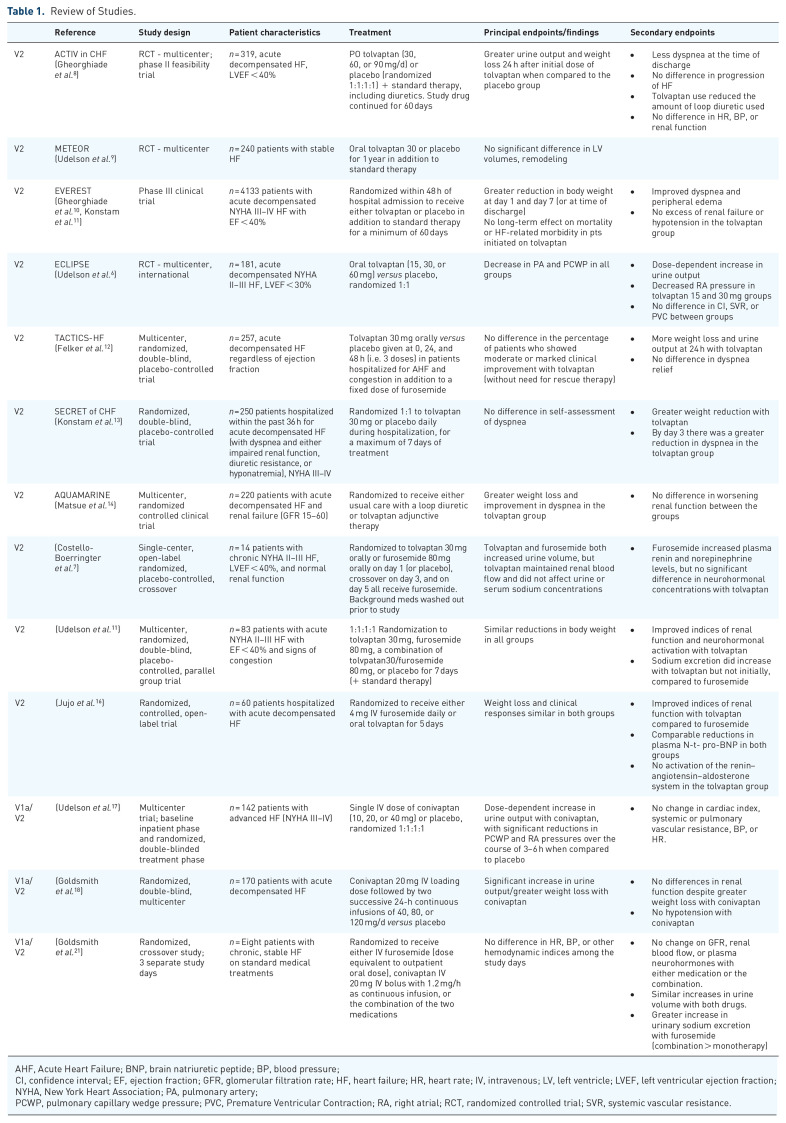
For decades, plasma arginine vasopressin (AVP) levels have been known to be elevated in patients with congestive heart failure (HF). Excessive AVP signaling at either or both the V1a and V2 receptors could contribute to the pathophysiology of HF by several mechanisms. V1a activation could cause vasoconstriction and/or direct myocardial hypertrophy as intracellular signaling pathways are closely related to those for angiotensin II. V2 activation could cause fluid retention and hyponatremia. A hemodynamic study with the pure V2 antagonist tolvaptan (TV) showed minimal hemodynamic effects. Compared with furosemide in another study, the renal and neurohormonal effects of TV were favorable. Several clinical trials with TV as adjunctive therapy in acute HF have shown beneficial effects on fluid balance and dyspnea, with no worsening of renal function or neurohormonal stimulation. Two smaller studies, one in acute and one in chronic HF, have shown comparable clinical and more favorable renal and neurohormonal effects of TV compared with loop diuretics. However, long-term treatment with TV did not alter outcomes in acute HF. No data are available other than single-dose studies of an intravenous pure V1a antagonist, which showed a vasodilating effect if plasma AVP levels were elevated. One hemodynamic study and one short-duration clinical trial with the balanced intravenous V1a/V2 antagonist conivaptan (CV) showed hemodynamic and clinical effects largely similar to those with TV in similar studies. A new orally effective balanced V1/V2 antagonist (pecavaptan) is currently undergoing phase II study as both adjunctive and alternative therapy during and after hospitalization for acute HF. The purpose of this review is to summarize what we have learned from the clinical experience with TV and CV, and to suggest implications of these findings for future work with newer agents.
期刊介绍:
The journal is aimed at clinicians and researchers from the cardiovascular disease field and will be a forum for all views and reviews relating to this discipline.Topics covered will include: ·arteriosclerosis ·cardiomyopathies ·coronary artery disease ·diabetes ·heart failure ·hypertension ·metabolic syndrome ·obesity ·peripheral arterial disease ·stroke ·arrhythmias ·genetics



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
