Jose C Alvarez-Payares, Marcel E Ribero, Sara Ramírez-Urrea, María C Fragozo-Ramos, Jose E Agámez-Gómez, Alejandro Román-González, Luis F Arias, Roberto Benavides Arenas, Fernando López-Urbano
{"title":"巨大甲状旁腺腺瘤相关骨折,并非所有溶解性骨病变都是癌症:一项基于病例的回顾。","authors":"Jose C Alvarez-Payares, Marcel E Ribero, Sara Ramírez-Urrea, María C Fragozo-Ramos, Jose E Agámez-Gómez, Alejandro Román-González, Luis F Arias, Roberto Benavides Arenas, Fernando López-Urbano","doi":"10.1155/2022/3969542","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Due to the early diagnosis of primary hyperparathyroidism the musculoskeletal manifestations of this disease are becoming less frequent. When this disease manifests secondary to a giant adenoma, it presents with more aggressive symptoms and can have important repercussions such as the hungry bone syndrome after parathyroidectomy. There are few reported cases of hyperparathyroidism secondary to a giant adenoma in the literature, as the presence of a brown tumor is often misinterpreted as a metastatic lesion from an unknown primary tumor.</p><p><strong>Methods: </strong>We describe a case and performed a literature review to identify all case reports. A literature search was carried out on PubMed/MEDLINE and EMBASE bibliographic databases. All available studies from May 2009 to May 2021 were included. Data were tabulated, and outcomes were cumulatively analyzed.</p><p><strong>Results: </strong>Twenty-four cases of primary hyperparathyroidism due to giant adenoma have been described; the majority were women, with a mean age of 52 years. They presented with heterogeneous symptoms such as palpable nodules (45%), bone pain (33%), brown tumor (12.5%), asymptomatic (12.5%), metabolic profile with a mean calcemia of 13.8 mg/dL, PTH 1109 ng/L, and mean tumor weight of 47.24 g.</p><p><strong>Conclusion: </strong>Primary hyperparathyroidism due to giant adenoma increases the risk of developing potentially serious postoperative complications such as hungry bone syndrome. This implies the need of implementing preventive measures comprising administration of intravenous zoledronic acid and early supplementation of oral calcium to prevent complications after resection.</p>","PeriodicalId":9627,"journal":{"name":"Case Reports in Medicine","volume":" ","pages":"3969542"},"PeriodicalIF":0.7000,"publicationDate":"2022-01-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8817849/pdf/","citationCount":"1","resultStr":"{\"title\":\"Giant Parathyroid Adenoma-Associated Fracture, Not All Lytic Bone Lesions are <i>Cancer</i>: A Case-Based Review.\",\"authors\":\"Jose C Alvarez-Payares, Marcel E Ribero, Sara Ramírez-Urrea, María C Fragozo-Ramos, Jose E Agámez-Gómez, Alejandro Román-González, Luis F Arias, Roberto Benavides Arenas, Fernando López-Urbano\",\"doi\":\"10.1155/2022/3969542\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Due to the early diagnosis of primary hyperparathyroidism the musculoskeletal manifestations of this disease are becoming less frequent. When this disease manifests secondary to a giant adenoma, it presents with more aggressive symptoms and can have important repercussions such as the hungry bone syndrome after parathyroidectomy. There are few reported cases of hyperparathyroidism secondary to a giant adenoma in the literature, as the presence of a brown tumor is often misinterpreted as a metastatic lesion from an unknown primary tumor.</p><p><strong>Methods: </strong>We describe a case and performed a literature review to identify all case reports. A literature search was carried out on PubMed/MEDLINE and EMBASE bibliographic databases. All available studies from May 2009 to May 2021 were included. Data were tabulated, and outcomes were cumulatively analyzed.</p><p><strong>Results: </strong>Twenty-four cases of primary hyperparathyroidism due to giant adenoma have been described; the majority were women, with a mean age of 52 years. They presented with heterogeneous symptoms such as palpable nodules (45%), bone pain (33%), brown tumor (12.5%), asymptomatic (12.5%), metabolic profile with a mean calcemia of 13.8 mg/dL, PTH 1109 ng/L, and mean tumor weight of 47.24 g.</p><p><strong>Conclusion: </strong>Primary hyperparathyroidism due to giant adenoma increases the risk of developing potentially serious postoperative complications such as hungry bone syndrome. This implies the need of implementing preventive measures comprising administration of intravenous zoledronic acid and early supplementation of oral calcium to prevent complications after resection.</p>\",\"PeriodicalId\":9627,\"journal\":{\"name\":\"Case Reports in Medicine\",\"volume\":\" \",\"pages\":\"3969542\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2022-01-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8817849/pdf/\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2022/3969542\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2022/3969542","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Giant Parathyroid Adenoma-Associated Fracture, Not All Lytic Bone Lesions are Cancer: A Case-Based Review.
Introduction: Due to the early diagnosis of primary hyperparathyroidism the musculoskeletal manifestations of this disease are becoming less frequent. When this disease manifests secondary to a giant adenoma, it presents with more aggressive symptoms and can have important repercussions such as the hungry bone syndrome after parathyroidectomy. There are few reported cases of hyperparathyroidism secondary to a giant adenoma in the literature, as the presence of a brown tumor is often misinterpreted as a metastatic lesion from an unknown primary tumor.
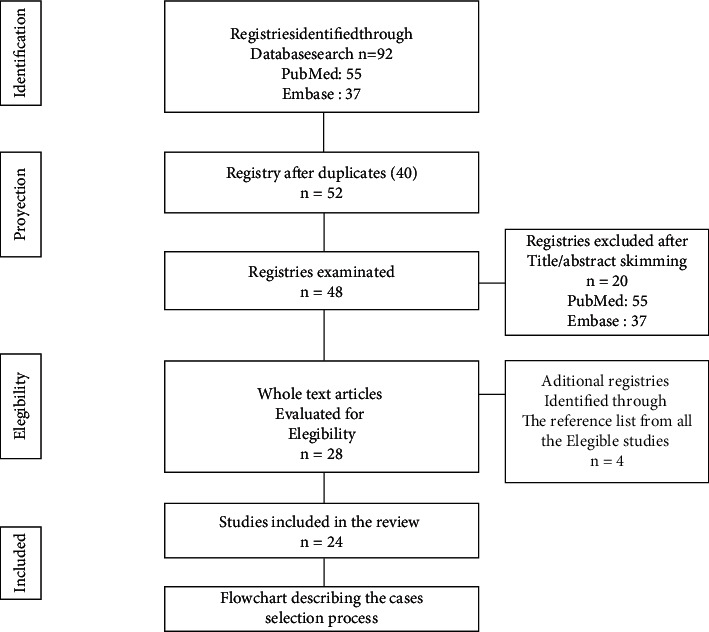
Methods: We describe a case and performed a literature review to identify all case reports. A literature search was carried out on PubMed/MEDLINE and EMBASE bibliographic databases. All available studies from May 2009 to May 2021 were included. Data were tabulated, and outcomes were cumulatively analyzed.
Results: Twenty-four cases of primary hyperparathyroidism due to giant adenoma have been described; the majority were women, with a mean age of 52 years. They presented with heterogeneous symptoms such as palpable nodules (45%), bone pain (33%), brown tumor (12.5%), asymptomatic (12.5%), metabolic profile with a mean calcemia of 13.8 mg/dL, PTH 1109 ng/L, and mean tumor weight of 47.24 g.
Conclusion: Primary hyperparathyroidism due to giant adenoma increases the risk of developing potentially serious postoperative complications such as hungry bone syndrome. This implies the need of implementing preventive measures comprising administration of intravenous zoledronic acid and early supplementation of oral calcium to prevent complications after resection.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
