{"title":"类风湿关节炎与银屑病关节炎腋窝淋巴结的ct比较。","authors":"Takeshi Fukuda, Reina Kayama, Sho Ogiwara, Takenori Yonenaga, Hiroya Ojiri","doi":"10.1177/20584601221112616","DOIUrl":null,"url":null,"abstract":"<p><strong>Backgrounds: </strong>There is a lack of universally available biomarker to differentiate rheumatoid arthritis (RA) and psoriatic arthritis (PsA).</p><p><strong>Purpose: </strong>to see if the size of the axillary lymphnodes (ALNs) and the frequency of lymphadenopathy are useful biomarker to differentiate RA and PsA.</p><p><strong>Material and methods: </strong>Forty RA and 19 PsA patients without previous biologics usage were retrospectively included. Chest CT was assessed for the presence of lymphadenopathy and the size of the largest ALN. Frequency of lymphadenopathies was statistically compared between RA and PsA. The short axis and the long axis of the largest ALN were also compared and receiver operating characteristic (ROC) curve analysis was performed.</p><p><strong>Results: </strong>Frequency of axillary lymphadenopathy was significantly higher in RA than in PsA (80% vs 31.6%, <i>p</i> < .001). Number of lymphadenopathies in each patient was also significantly higher in RA than in PsA (3.0 vs 1.2 per patient, <i>p</i> = .005). Sensitivity and specificity for differentiating RA from PsA by the presence of at least one axillary lymphadenopathy were 0.8 and 0.68, respectively.The short axis of the largest ALNs in RA was significantly longer than in PsA (6.5 ± 1.6 mm vs 4.7 ± 1.7 mm, <i>p</i> < .001). ROC curve analysis of the short axis showed AUC of 0.75 (<i>p</i> = .002) and the cutoff value of 5.1 mm with a sensitivity of 0.83 and specificity of 0.74, when differentiating RA and PsA.</p><p><strong>Conclusion: </strong>Presence of ALN lymphadenopathy and the short axis of the largest ALN may have a potential utility in differentiating RA and PsA.</p>","PeriodicalId":72063,"journal":{"name":"Acta radiologica open","volume":null,"pages":null},"PeriodicalIF":0.9000,"publicationDate":"2022-07-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/37/59/10.1177_20584601221112616.PMC9284224.pdf","citationCount":"0","resultStr":"{\"title\":\"Comparison of the axillary lymph node between rheumatoid arthritis and psoriatic arthritis with computed tomography.\",\"authors\":\"Takeshi Fukuda, Reina Kayama, Sho Ogiwara, Takenori Yonenaga, Hiroya Ojiri\",\"doi\":\"10.1177/20584601221112616\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Backgrounds: </strong>There is a lack of universally available biomarker to differentiate rheumatoid arthritis (RA) and psoriatic arthritis (PsA).</p><p><strong>Purpose: </strong>to see if the size of the axillary lymphnodes (ALNs) and the frequency of lymphadenopathy are useful biomarker to differentiate RA and PsA.</p><p><strong>Material and methods: </strong>Forty RA and 19 PsA patients without previous biologics usage were retrospectively included. Chest CT was assessed for the presence of lymphadenopathy and the size of the largest ALN. Frequency of lymphadenopathies was statistically compared between RA and PsA. The short axis and the long axis of the largest ALN were also compared and receiver operating characteristic (ROC) curve analysis was performed.</p><p><strong>Results: </strong>Frequency of axillary lymphadenopathy was significantly higher in RA than in PsA (80% vs 31.6%, <i>p</i> < .001). Number of lymphadenopathies in each patient was also significantly higher in RA than in PsA (3.0 vs 1.2 per patient, <i>p</i> = .005). Sensitivity and specificity for differentiating RA from PsA by the presence of at least one axillary lymphadenopathy were 0.8 and 0.68, respectively.The short axis of the largest ALNs in RA was significantly longer than in PsA (6.5 ± 1.6 mm vs 4.7 ± 1.7 mm, <i>p</i> < .001). ROC curve analysis of the short axis showed AUC of 0.75 (<i>p</i> = .002) and the cutoff value of 5.1 mm with a sensitivity of 0.83 and specificity of 0.74, when differentiating RA and PsA.</p><p><strong>Conclusion: </strong>Presence of ALN lymphadenopathy and the short axis of the largest ALN may have a potential utility in differentiating RA and PsA.</p>\",\"PeriodicalId\":72063,\"journal\":{\"name\":\"Acta radiologica open\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2022-07-13\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/37/59/10.1177_20584601221112616.PMC9284224.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Acta radiologica open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20584601221112616\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2022/7/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Acta radiologica open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20584601221112616","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/7/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
引用次数: 0
摘要
背景:类风湿关节炎(RA)和银屑病关节炎(PsA)缺乏普遍可用的生物标志物来区分。目的:探讨腋窝淋巴结(ALNs)的大小和淋巴结病变的频率是否可作为鉴别RA和PsA的有用生物标志物。材料和方法:回顾性分析40例RA和19例PsA患者,既往未使用过生物制剂。胸部CT检查是否有淋巴结病变和最大ALN的大小。对RA和PsA的淋巴结病变频率进行统计学比较。比较最大ALN的短轴和长轴,并进行受试者工作特征(ROC)曲线分析。结果:RA患者腋窝淋巴结病变发生率明显高于PsA患者(80% vs 31.6%, p < 0.001)。RA患者中每个患者的淋巴结病变数量也显著高于PsA患者(每个患者3.0 vs 1.2, p = 0.005)。通过存在至少一个腋窝淋巴结病变来区分RA和PsA的敏感性和特异性分别为0.8和0.68。RA组最大aln的短轴明显长于PsA组(6.5±1.6 mm vs 4.7±1.7 mm, p < 0.001)。短轴ROC曲线分析显示,鉴别RA与PsA的AUC为0.75 (p = 0.002), cut - off值为5.1 mm,敏感性为0.83,特异性为0.74。结论:ALN淋巴结病变的存在和最大ALN的短轴可能对RA和PsA的鉴别有潜在的价值。
Comparison of the axillary lymph node between rheumatoid arthritis and psoriatic arthritis with computed tomography.
Backgrounds: There is a lack of universally available biomarker to differentiate rheumatoid arthritis (RA) and psoriatic arthritis (PsA).
Purpose: to see if the size of the axillary lymphnodes (ALNs) and the frequency of lymphadenopathy are useful biomarker to differentiate RA and PsA.
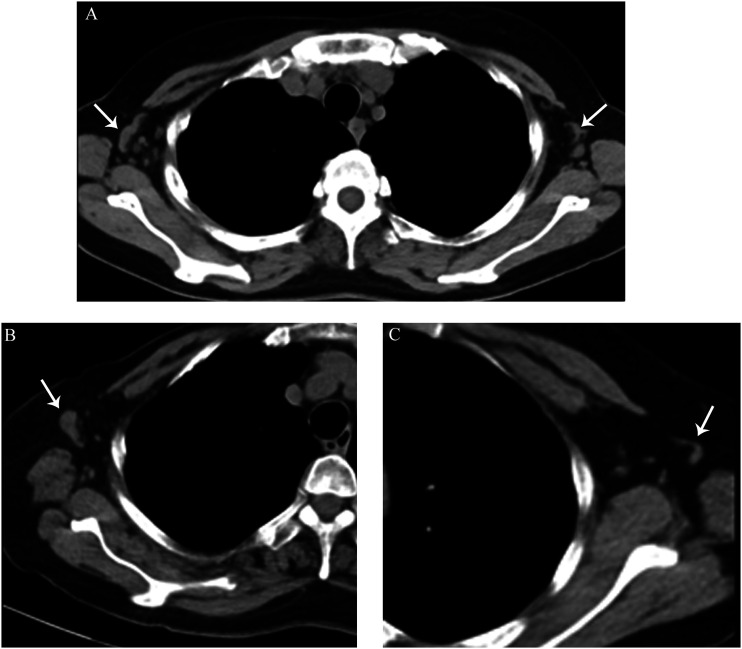
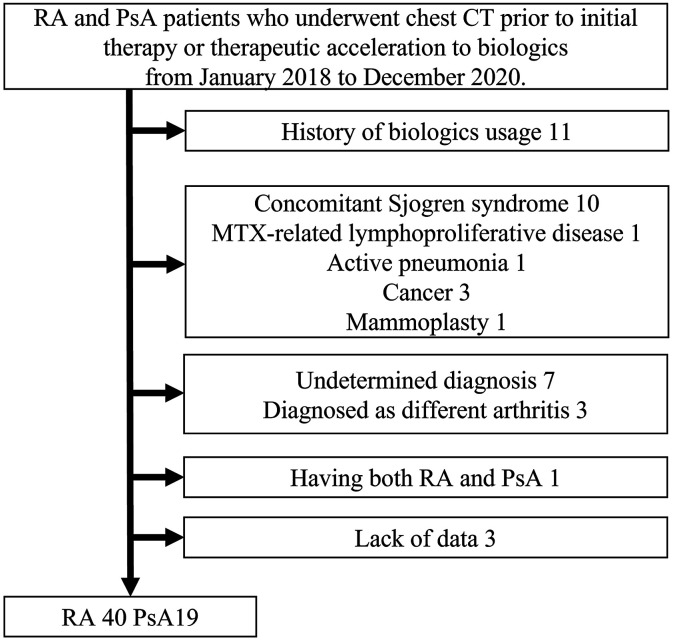
Material and methods: Forty RA and 19 PsA patients without previous biologics usage were retrospectively included. Chest CT was assessed for the presence of lymphadenopathy and the size of the largest ALN. Frequency of lymphadenopathies was statistically compared between RA and PsA. The short axis and the long axis of the largest ALN were also compared and receiver operating characteristic (ROC) curve analysis was performed.
Results: Frequency of axillary lymphadenopathy was significantly higher in RA than in PsA (80% vs 31.6%, p < .001). Number of lymphadenopathies in each patient was also significantly higher in RA than in PsA (3.0 vs 1.2 per patient, p = .005). Sensitivity and specificity for differentiating RA from PsA by the presence of at least one axillary lymphadenopathy were 0.8 and 0.68, respectively.The short axis of the largest ALNs in RA was significantly longer than in PsA (6.5 ± 1.6 mm vs 4.7 ± 1.7 mm, p < .001). ROC curve analysis of the short axis showed AUC of 0.75 (p = .002) and the cutoff value of 5.1 mm with a sensitivity of 0.83 and specificity of 0.74, when differentiating RA and PsA.
Conclusion: Presence of ALN lymphadenopathy and the short axis of the largest ALN may have a potential utility in differentiating RA and PsA.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
