{"title":"颅内出血后2周内开始抗凝是否安全:一项系统回顾和荟萃分析","authors":"Xue-Yan Huang, Jun-Yan Zhang, Chang-Yin Yu","doi":"10.1002/ibra.12060","DOIUrl":null,"url":null,"abstract":"<p>Whether restarting anticoagulation (RA) treatment after intracranial hemorrhage (ICH) is still controversial. We performed a systematic review and meta-analysis to summarize the relationship between anticoagulation after ICH with the recurrence of hemorrhagic events, ischemic events, and long-term mortality. Medline, Embase, and the Cochrane Central Register of Controlled Trials, from inception to November 2020. We searched the published medical literature to ensure cohort studies involving ICH associated with anticoagulation in adults. Primary outcomes were long-term mortality, hemorrhagic events, and ischemic events (myocardial infarction, pulmonary embolism, ischemic stroke, or systemic embolization). We concluded seven retrospective cohorts, including 1876 intracranial hemorrhage patients with indications of anticoagulation. The ratio of the anticoagulant restart was 35.3% (664n). RA was associated with a significantly lower incidence of recurrent ischemic events (pooled odds ratio [OR] 0.29, 95% confidence interval [CI] 0.19% to 0.45%, <i>p</i> = 0.97) and death events (pooled OR 0.56, 95% CI 0.40%–0.79%, <i>p</i> = 0.27). There is no evidence that early recovery of anticoagulation (within 2 weeks or 1 month) is associated with the occurrence of hemorrhagic events (within 2 weeks: pooled OR 0.80, 95% CI 0.3–2.12, <i>p</i> = 0.52 vs. within 1 month: pooled OR 1.14, 95% CI 0.77–1.68, <i>p</i> = 0.82). Based on these, recovery of anticoagulation after ICH is beneficial for long-term mortality and recurrence of ischemic events. The meta-analysis showed a resumption of oral anticoagulation within 2 weeks or 1 month in patients who had a cerebral hemorrhage was beneficial and did not increase the risk of hemorrhagic events and reduced the occurrence of ischemic and fatal endpoint events.</p>","PeriodicalId":94030,"journal":{"name":"Ibrain","volume":"8 3","pages":"377-388"},"PeriodicalIF":0.0000,"publicationDate":"2022-08-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10528763/pdf/","citationCount":"0","resultStr":"{\"title\":\"Whether it is safe to start anticoagulation after intracranial hemorrhage within 2 weeks: A systematic review and meta-analysis\",\"authors\":\"Xue-Yan Huang, Jun-Yan Zhang, Chang-Yin Yu\",\"doi\":\"10.1002/ibra.12060\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Whether restarting anticoagulation (RA) treatment after intracranial hemorrhage (ICH) is still controversial. We performed a systematic review and meta-analysis to summarize the relationship between anticoagulation after ICH with the recurrence of hemorrhagic events, ischemic events, and long-term mortality. Medline, Embase, and the Cochrane Central Register of Controlled Trials, from inception to November 2020. We searched the published medical literature to ensure cohort studies involving ICH associated with anticoagulation in adults. Primary outcomes were long-term mortality, hemorrhagic events, and ischemic events (myocardial infarction, pulmonary embolism, ischemic stroke, or systemic embolization). We concluded seven retrospective cohorts, including 1876 intracranial hemorrhage patients with indications of anticoagulation. The ratio of the anticoagulant restart was 35.3% (664n). RA was associated with a significantly lower incidence of recurrent ischemic events (pooled odds ratio [OR] 0.29, 95% confidence interval [CI] 0.19% to 0.45%, <i>p</i> = 0.97) and death events (pooled OR 0.56, 95% CI 0.40%–0.79%, <i>p</i> = 0.27). There is no evidence that early recovery of anticoagulation (within 2 weeks or 1 month) is associated with the occurrence of hemorrhagic events (within 2 weeks: pooled OR 0.80, 95% CI 0.3–2.12, <i>p</i> = 0.52 vs. within 1 month: pooled OR 1.14, 95% CI 0.77–1.68, <i>p</i> = 0.82). Based on these, recovery of anticoagulation after ICH is beneficial for long-term mortality and recurrence of ischemic events. The meta-analysis showed a resumption of oral anticoagulation within 2 weeks or 1 month in patients who had a cerebral hemorrhage was beneficial and did not increase the risk of hemorrhagic events and reduced the occurrence of ischemic and fatal endpoint events.</p>\",\"PeriodicalId\":94030,\"journal\":{\"name\":\"Ibrain\",\"volume\":\"8 3\",\"pages\":\"377-388\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-08-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10528763/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Ibrain\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ibra.12060\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ibrain","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ibra.12060","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
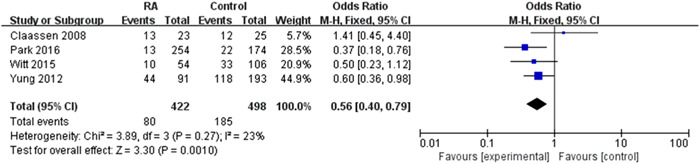
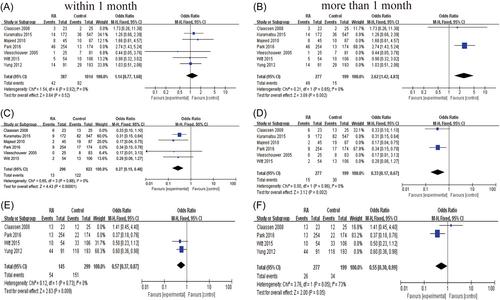
颅内出血(ICH)后是否重新开始抗凝治疗(RA)仍存在争议。我们进行了系统回顾和荟萃分析,以总结脑出血后抗凝与出血事件复发、缺血事件和长期死亡率之间的关系。Medline, Embase和Cochrane Central Register of Controlled Trials,从成立到2020年11月。我们检索了已发表的医学文献,以确保涉及脑出血与成人抗凝相关的队列研究。主要结局是长期死亡率、出血性事件和缺血性事件(心肌梗死、肺栓塞、缺血性中风或全身栓塞)。我们总结了7个回顾性队列,包括1876例有抗凝指征的颅内出血患者。抗凝药重启率为35.3% (664n)。RA与复发性缺血性事件(合并优势比[OR] 0.29, 95%可信区间[CI] 0.19% ~ 0.45%, p = 0.97)和死亡事件(合并优势比[OR] 0.56, 95% CI 0.40% ~ 0.79%, p = 0.27)的发生率显著降低相关。没有证据表明抗凝治疗的早期恢复(2周或1个月内)与出血事件的发生有关(2周内:合并or为0.80,95% CI为0.3-2.12,p = 0.52; 1个月内:合并or为1.14,95% CI为0.77-1.68,p = 0.82)。基于这些,脑出血后抗凝治疗的恢复有利于长期死亡率和缺血性事件的复发。荟萃分析显示,脑出血患者在2周或1个月内恢复口服抗凝治疗是有益的,不会增加出血事件的风险,并减少缺血性和致命终点事件的发生。
Whether it is safe to start anticoagulation after intracranial hemorrhage within 2 weeks: A systematic review and meta-analysis
Whether restarting anticoagulation (RA) treatment after intracranial hemorrhage (ICH) is still controversial. We performed a systematic review and meta-analysis to summarize the relationship between anticoagulation after ICH with the recurrence of hemorrhagic events, ischemic events, and long-term mortality. Medline, Embase, and the Cochrane Central Register of Controlled Trials, from inception to November 2020. We searched the published medical literature to ensure cohort studies involving ICH associated with anticoagulation in adults. Primary outcomes were long-term mortality, hemorrhagic events, and ischemic events (myocardial infarction, pulmonary embolism, ischemic stroke, or systemic embolization). We concluded seven retrospective cohorts, including 1876 intracranial hemorrhage patients with indications of anticoagulation. The ratio of the anticoagulant restart was 35.3% (664n). RA was associated with a significantly lower incidence of recurrent ischemic events (pooled odds ratio [OR] 0.29, 95% confidence interval [CI] 0.19% to 0.45%, p = 0.97) and death events (pooled OR 0.56, 95% CI 0.40%–0.79%, p = 0.27). There is no evidence that early recovery of anticoagulation (within 2 weeks or 1 month) is associated with the occurrence of hemorrhagic events (within 2 weeks: pooled OR 0.80, 95% CI 0.3–2.12, p = 0.52 vs. within 1 month: pooled OR 1.14, 95% CI 0.77–1.68, p = 0.82). Based on these, recovery of anticoagulation after ICH is beneficial for long-term mortality and recurrence of ischemic events. The meta-analysis showed a resumption of oral anticoagulation within 2 weeks or 1 month in patients who had a cerebral hemorrhage was beneficial and did not increase the risk of hemorrhagic events and reduced the occurrence of ischemic and fatal endpoint events.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
