Aslam Amod, John B Buse, Darren K McGuire, Thomas R Pieber, Rodica Pop-Busui, Richard E Pratley, Bernard Zinman, Marco Bo Hansen, Ting Jia, Thomas Mark, Neil R Poulter
{"title":"2型糖尿病患者肾小球滤过率与心血管事件、死亡率和严重低血糖的相关风险:次要分析","authors":"Aslam Amod, John B Buse, Darren K McGuire, Thomas R Pieber, Rodica Pop-Busui, Richard E Pratley, Bernard Zinman, Marco Bo Hansen, Ting Jia, Thomas Mark, Neil R Poulter","doi":"10.1007/s13300-019-00715-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The associations of chronic kidney disease (CKD) severity, cardiovascular disease (CVD), and insulin with the risks of major adverse cardiovascular events (MACE), mortality, and severe hypoglycemia in patients with type 2 diabetes (T2D) at high cardiovascular (CV) risk are not known. This secondary, pooled analysis of data from the DEVOTE trial examined whether baseline glomerular filtration rate (GFR) categories were associated with a higher risk of these outcomes.</p><p><strong>Methods: </strong>DEVOTE was a treat-to-target, double-blind trial involving 7637 patients with T2D at high CV risk who were randomized to once-daily treatment with either insulin degludec (degludec) or insulin glargine 100 units/mL (glargine U100). Patients with estimated GFR data at baseline (n = 7522) were analyzed following stratification into four GFR categories.</p><p><strong>Results: </strong>The risks of MACE, CV death, and all-cause mortality increased with worsening baseline GFR category (P < 0.05), with a trend towards higher rates of severe hypoglycemia. Patients with prior CVD, CKD (estimated GFR < 60 mL/min/m<sup>2</sup>), or both were at higher risk of MACE, CV death, and all-cause mortality. Only CKD was associated with a higher rate of severe hypoglycemia, and the risk of MACE was higher in patients with CVD than in those with CKD (P = 0.0003). There were no significant interactions between randomized treatment and GFR category.</p><p><strong>Conclusion: </strong>The risks of MACE, CV death, and all-cause mortality were higher with lower baseline GFR and with prior CVD, CKD, or both. The relative effects of degludec versus glargine U100 on outcomes were consistent across baseline GFR categories, suggesting that the lower rate of severe hypoglycemia associated with degludec use versus glargine U100 use was independent of baseline GFR category.</p><p><strong>Funding: </strong>Novo Nordisk.</p>","PeriodicalId":48675,"journal":{"name":"Diabetes Therapy","volume":"11 1","pages":"53-70"},"PeriodicalIF":2.6000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6974100/pdf/","citationCount":"0","resultStr":"{\"title\":\"Glomerular Filtration Rate and Associated Risks of Cardiovascular Events, Mortality, and Severe Hypoglycemia in Patients with Type 2 Diabetes: Secondary Analysis (DEVOTE 11).\",\"authors\":\"Aslam Amod, John B Buse, Darren K McGuire, Thomas R Pieber, Rodica Pop-Busui, Richard E Pratley, Bernard Zinman, Marco Bo Hansen, Ting Jia, Thomas Mark, Neil R Poulter\",\"doi\":\"10.1007/s13300-019-00715-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>The associations of chronic kidney disease (CKD) severity, cardiovascular disease (CVD), and insulin with the risks of major adverse cardiovascular events (MACE), mortality, and severe hypoglycemia in patients with type 2 diabetes (T2D) at high cardiovascular (CV) risk are not known. This secondary, pooled analysis of data from the DEVOTE trial examined whether baseline glomerular filtration rate (GFR) categories were associated with a higher risk of these outcomes.</p><p><strong>Methods: </strong>DEVOTE was a treat-to-target, double-blind trial involving 7637 patients with T2D at high CV risk who were randomized to once-daily treatment with either insulin degludec (degludec) or insulin glargine 100 units/mL (glargine U100). Patients with estimated GFR data at baseline (n = 7522) were analyzed following stratification into four GFR categories.</p><p><strong>Results: </strong>The risks of MACE, CV death, and all-cause mortality increased with worsening baseline GFR category (P < 0.05), with a trend towards higher rates of severe hypoglycemia. Patients with prior CVD, CKD (estimated GFR < 60 mL/min/m<sup>2</sup>), or both were at higher risk of MACE, CV death, and all-cause mortality. Only CKD was associated with a higher rate of severe hypoglycemia, and the risk of MACE was higher in patients with CVD than in those with CKD (P = 0.0003). There were no significant interactions between randomized treatment and GFR category.</p><p><strong>Conclusion: </strong>The risks of MACE, CV death, and all-cause mortality were higher with lower baseline GFR and with prior CVD, CKD, or both. The relative effects of degludec versus glargine U100 on outcomes were consistent across baseline GFR categories, suggesting that the lower rate of severe hypoglycemia associated with degludec use versus glargine U100 use was independent of baseline GFR category.</p><p><strong>Funding: </strong>Novo Nordisk.</p>\",\"PeriodicalId\":48675,\"journal\":{\"name\":\"Diabetes Therapy\",\"volume\":\"11 1\",\"pages\":\"53-70\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2020-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6974100/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diabetes Therapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s13300-019-00715-x\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2019/10/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"ENDOCRINOLOGY & METABOLISM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diabetes Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s13300-019-00715-x","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2019/10/30 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
摘要
导言:慢性肾脏病(CKD)严重程度、心血管疾病(CVD)和胰岛素与心血管疾病(CV)高风险2型糖尿病(T2D)患者的主要不良心血管事件(MACE)、死亡率和严重低血糖风险之间的关系尚不清楚。这项对 DEVOTE 试验数据进行的二次汇总分析研究了基线肾小球滤过率(GFR)类别是否与这些结果的较高风险相关:DEVOTE是一项按目标治疗的双盲试验,共有7637名具有高CV风险的T2D患者参与,他们被随机分配接受胰岛素degludec(degludec)或胰岛素glargine 100单位/毫升(glargine U100)的每日一次治疗。将基线时有估计 GFR 数据的患者(n = 7522)分为四个 GFR 类别进行分析:结果:MACE、CV 死亡和全因死亡的风险随着基线 GFR 类别的恶化而增加(P 2),或者两者的 MACE、CV 死亡和全因死亡风险都较高。只有慢性肾脏病与较高的严重低血糖发生率相关,心血管疾病患者的 MACE 风险高于慢性肾脏病患者(P = 0.0003)。随机治疗与 GFR 类别之间没有明显的相互作用:结论:MACE、心血管疾病死亡和全因死亡的风险在基线 GFR 较低以及既往患有心血管疾病、慢性肾脏病或两者兼有的情况下更高。degludec与glargine U100对不同基线GFR类别结果的相对影响是一致的,这表明使用degludec与使用glargine U100相关的严重低血糖发生率较低与基线GFR类别无关:诺和诺德公司。
Glomerular Filtration Rate and Associated Risks of Cardiovascular Events, Mortality, and Severe Hypoglycemia in Patients with Type 2 Diabetes: Secondary Analysis (DEVOTE 11).
Introduction: The associations of chronic kidney disease (CKD) severity, cardiovascular disease (CVD), and insulin with the risks of major adverse cardiovascular events (MACE), mortality, and severe hypoglycemia in patients with type 2 diabetes (T2D) at high cardiovascular (CV) risk are not known. This secondary, pooled analysis of data from the DEVOTE trial examined whether baseline glomerular filtration rate (GFR) categories were associated with a higher risk of these outcomes.
Methods: DEVOTE was a treat-to-target, double-blind trial involving 7637 patients with T2D at high CV risk who were randomized to once-daily treatment with either insulin degludec (degludec) or insulin glargine 100 units/mL (glargine U100). Patients with estimated GFR data at baseline (n = 7522) were analyzed following stratification into four GFR categories.
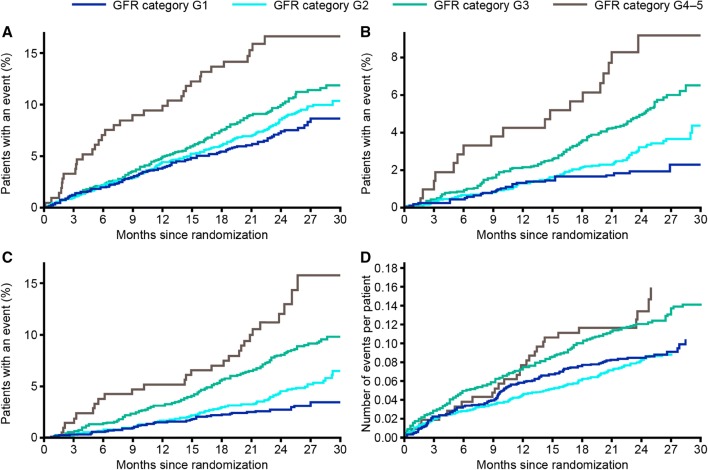
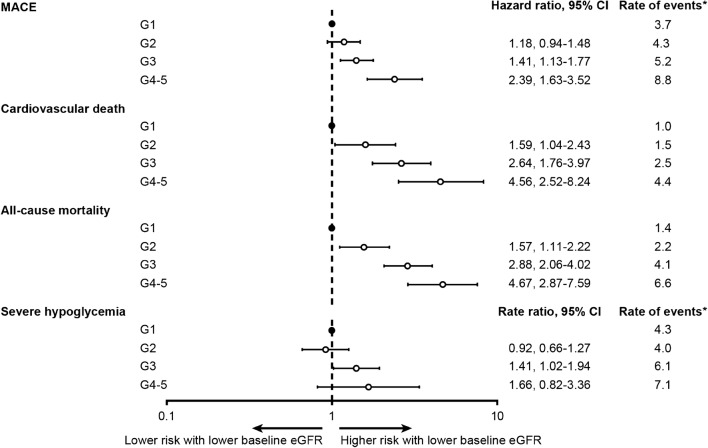
Results: The risks of MACE, CV death, and all-cause mortality increased with worsening baseline GFR category (P < 0.05), with a trend towards higher rates of severe hypoglycemia. Patients with prior CVD, CKD (estimated GFR < 60 mL/min/m2), or both were at higher risk of MACE, CV death, and all-cause mortality. Only CKD was associated with a higher rate of severe hypoglycemia, and the risk of MACE was higher in patients with CVD than in those with CKD (P = 0.0003). There were no significant interactions between randomized treatment and GFR category.
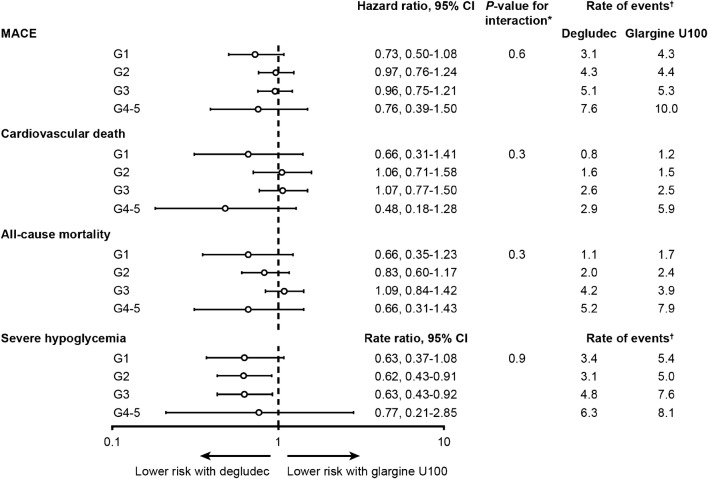
Conclusion: The risks of MACE, CV death, and all-cause mortality were higher with lower baseline GFR and with prior CVD, CKD, or both. The relative effects of degludec versus glargine U100 on outcomes were consistent across baseline GFR categories, suggesting that the lower rate of severe hypoglycemia associated with degludec use versus glargine U100 use was independent of baseline GFR category.
期刊介绍:
Diabetes Therapy is an international, peer reviewed, rapid-publication (peer review in 2 weeks, published 3–4 weeks from acceptance) journal dedicated to the publication of high-quality clinical (all phases), observational, real-world, and health outcomes research around the discovery, development, and use of therapeutics and interventions (including devices) across all areas of diabetes. Studies relating to diagnostics and diagnosis, pharmacoeconomics, public health, epidemiology, quality of life, and patient care, management, and education are also encouraged.
The journal is of interest to a broad audience of healthcare professionals and publishes original research, reviews, communications and letters. The journal is read by a global audience and receives submissions from all over the world. Diabetes Therapy will consider all scientifically sound research be it positive, confirmatory or negative data. Submissions are welcomed whether they relate to an international and/or a country-specific audience, something that is crucially important when researchers are trying to target more specific patient populations. This inclusive approach allows the journal to assist in the dissemination of all scientifically and ethically sound research.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
