{"title":"弥漫性大b细胞淋巴瘤的起源细胞分类。","authors":"Lity Dhar, Sarika Singh, Shyam Lata Jain, Anubhav Vindal, Pallavi Sinha, Rashmi Gautam","doi":"10.4103/jmau.jmau_66_22","DOIUrl":null,"url":null,"abstract":"<p><strong>Context: </strong>Diffuse large B-cell lymphoma (DLBCL) is a neoplasm of medium-to-large B lymphoid cells with diffuse growth patterns. Although it is a potentially curable disease, around 40% of the cases are either refractory to primary treatment or relapse. Based on gene expression profiling (GEP), DLBCL can be classified as germinal center B-cell subtype (GCB) and activated B-cell subtype (ABC). About 10%-15% of cases do not convincingly fall into either of the two subtypes and hence remain unclassified. Most widely used and suggested by WHO is Hans algorithm comprising immunohistochemical markers CD10, B-cell lymphoma6 (BCL6), and IRF4/MUM1, which classifies CD10+ and CD10-/BCL6+/MUM1-DLBCL as GCB, while CD10-/BCL6+/MUM1 + and BCL6-DLBCL as non-GCB.</p><p><strong>Aims: </strong>The aim of this study was to classify DLBCL into GCB and non-GCB subtypes using Hans Algorithm.</p><p><strong>Settings and design: </strong>This was a retrospective study.</p><p><strong>Materials and methods: </strong>Twenty-eight histologically diagnosed cases of nodal (71.4%), as well as extranodal (28.6%) DLBCL, were taken over the period of 2 years with age ranging between 10 and 65 years with 19 males and 9 females. M: F = 2.1:1. Depending upon the site involved, a primary panel of immunohistochemistry (IHC) markers, namely CD20, CD3, LCA, EMA, and CK, followed by a secondary panel comprising CD10, CD19, CD30, LMP1, BCL2, BCL6, MUM1, MYC, and FOXP1 was used.</p><p><strong>Results: </strong>In this study, it was found that the non-GCB subtype was more common than the GCB subtype in Indian population.</p><p><strong>Conclusions: </strong>Although the gold standard of GEP to assign cells of origin is using RNA microarray analysis, however, due to resource constraints and other limitations such as long turnaround times, IHC is the next acceptable alternative.</p>","PeriodicalId":16340,"journal":{"name":"Journal of Microscopy and Ultrastructure","volume":"1 1","pages":"193-198"},"PeriodicalIF":0.0000,"publicationDate":"2023-01-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11729026/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cell of Origin Classification of Diffuse Large B-Cell Lymphoma.\",\"authors\":\"Lity Dhar, Sarika Singh, Shyam Lata Jain, Anubhav Vindal, Pallavi Sinha, Rashmi Gautam\",\"doi\":\"10.4103/jmau.jmau_66_22\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Context: </strong>Diffuse large B-cell lymphoma (DLBCL) is a neoplasm of medium-to-large B lymphoid cells with diffuse growth patterns. Although it is a potentially curable disease, around 40% of the cases are either refractory to primary treatment or relapse. Based on gene expression profiling (GEP), DLBCL can be classified as germinal center B-cell subtype (GCB) and activated B-cell subtype (ABC). About 10%-15% of cases do not convincingly fall into either of the two subtypes and hence remain unclassified. Most widely used and suggested by WHO is Hans algorithm comprising immunohistochemical markers CD10, B-cell lymphoma6 (BCL6), and IRF4/MUM1, which classifies CD10+ and CD10-/BCL6+/MUM1-DLBCL as GCB, while CD10-/BCL6+/MUM1 + and BCL6-DLBCL as non-GCB.</p><p><strong>Aims: </strong>The aim of this study was to classify DLBCL into GCB and non-GCB subtypes using Hans Algorithm.</p><p><strong>Settings and design: </strong>This was a retrospective study.</p><p><strong>Materials and methods: </strong>Twenty-eight histologically diagnosed cases of nodal (71.4%), as well as extranodal (28.6%) DLBCL, were taken over the period of 2 years with age ranging between 10 and 65 years with 19 males and 9 females. M: F = 2.1:1. Depending upon the site involved, a primary panel of immunohistochemistry (IHC) markers, namely CD20, CD3, LCA, EMA, and CK, followed by a secondary panel comprising CD10, CD19, CD30, LMP1, BCL2, BCL6, MUM1, MYC, and FOXP1 was used.</p><p><strong>Results: </strong>In this study, it was found that the non-GCB subtype was more common than the GCB subtype in Indian population.</p><p><strong>Conclusions: </strong>Although the gold standard of GEP to assign cells of origin is using RNA microarray analysis, however, due to resource constraints and other limitations such as long turnaround times, IHC is the next acceptable alternative.</p>\",\"PeriodicalId\":16340,\"journal\":{\"name\":\"Journal of Microscopy and Ultrastructure\",\"volume\":\"1 1\",\"pages\":\"193-198\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-01-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11729026/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Microscopy and Ultrastructure\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.4103/jmau.jmau_66_22\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Microscopy and Ultrastructure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/jmau.jmau_66_22","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
摘要
背景:弥漫性大B细胞淋巴瘤(DLBCL)是一种具有弥漫性生长模式的大中型B淋巴样细胞肿瘤。虽然这是一种潜在的可治愈的疾病,但大约40%的病例要么对初级治疗难以治愈,要么复发。根据基因表达谱(GEP),可将DLBCL分为生发中心b细胞亚型(GCB)和活化b细胞亚型(ABC)。大约10%-15%的病例不能令人信服地属于两种亚型中的任何一种,因此仍未分类。WHO建议使用最广泛的是由免疫组织化学标记CD10、b细胞淋巴瘤6 (BCL6)和IRF4/MUM1组成的Hans算法,该算法将CD10+和CD10-/BCL6+/MUM1- dlbcl分类为GCB,而将CD10-/BCL6+/MUM1 +和BCL6- dlbcl分类为非GCB。目的:本研究采用Hans算法将DLBCL分为GCB亚型和非GCB亚型。环境和设计:这是一项回顾性研究。材料与方法:回顾性分析了28例经组织学诊断为结性DLBCL(71.4%)和结外DLBCL(28.6%)的病例,年龄10 ~ 65岁,男19例,女9例。M: f = 2.1:1。根据所涉及的部位,使用免疫组织化学(IHC)标记的初级组,即CD20、CD3、LCA、EMA和CK,其次使用包括CD10、CD19、CD30、LMP1、BCL2、BCL6、MUM1、MYC和FOXP1的次级组。结果:本研究发现印度人群中非GCB亚型比GCB亚型更为常见。结论:尽管使用RNA微阵列分析是GEP确定细胞来源的金标准,但是,由于资源限制和其他限制,如较长的周转时间,IHC是下一个可接受的选择。
Cell of Origin Classification of Diffuse Large B-Cell Lymphoma.
Context: Diffuse large B-cell lymphoma (DLBCL) is a neoplasm of medium-to-large B lymphoid cells with diffuse growth patterns. Although it is a potentially curable disease, around 40% of the cases are either refractory to primary treatment or relapse. Based on gene expression profiling (GEP), DLBCL can be classified as germinal center B-cell subtype (GCB) and activated B-cell subtype (ABC). About 10%-15% of cases do not convincingly fall into either of the two subtypes and hence remain unclassified. Most widely used and suggested by WHO is Hans algorithm comprising immunohistochemical markers CD10, B-cell lymphoma6 (BCL6), and IRF4/MUM1, which classifies CD10+ and CD10-/BCL6+/MUM1-DLBCL as GCB, while CD10-/BCL6+/MUM1 + and BCL6-DLBCL as non-GCB.
Aims: The aim of this study was to classify DLBCL into GCB and non-GCB subtypes using Hans Algorithm.
Settings and design: This was a retrospective study.
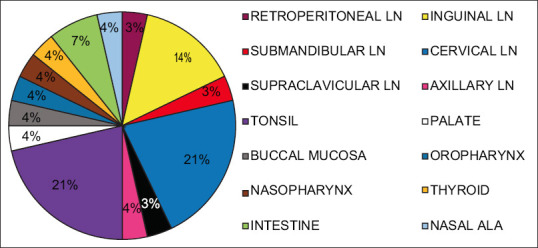
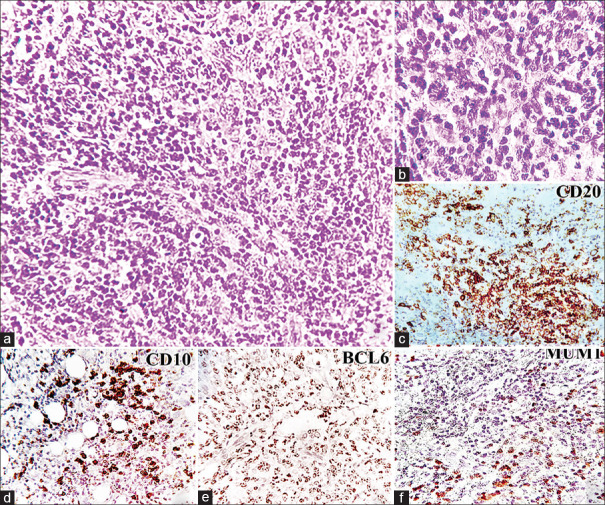
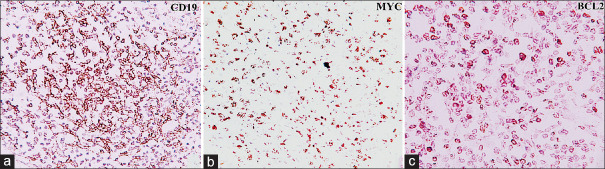
Materials and methods: Twenty-eight histologically diagnosed cases of nodal (71.4%), as well as extranodal (28.6%) DLBCL, were taken over the period of 2 years with age ranging between 10 and 65 years with 19 males and 9 females. M: F = 2.1:1. Depending upon the site involved, a primary panel of immunohistochemistry (IHC) markers, namely CD20, CD3, LCA, EMA, and CK, followed by a secondary panel comprising CD10, CD19, CD30, LMP1, BCL2, BCL6, MUM1, MYC, and FOXP1 was used.
Results: In this study, it was found that the non-GCB subtype was more common than the GCB subtype in Indian population.
Conclusions: Although the gold standard of GEP to assign cells of origin is using RNA microarray analysis, however, due to resource constraints and other limitations such as long turnaround times, IHC is the next acceptable alternative.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
