Laura Carrión, Ana Clemente-Sánchez, Laura Márquez-Pérez, Javier Orcajo-Rincón, Amanda Rotger, Enrique Ramón-Botella, Manuel González-Leyte, Miguel Echenagusía-Boyra, Arturo Luis Colón, Laura Reguera-Berenguer, Rafael Bañares, Diego Rincón, Ana Matilla-Peña
{"title":"门静脉高压增加肝细胞癌患者90Y放射性栓塞后肝功能失代偿的风险:一项队列研究。","authors":"Laura Carrión, Ana Clemente-Sánchez, Laura Márquez-Pérez, Javier Orcajo-Rincón, Amanda Rotger, Enrique Ramón-Botella, Manuel González-Leyte, Miguel Echenagusía-Boyra, Arturo Luis Colón, Laura Reguera-Berenguer, Rafael Bañares, Diego Rincón, Ana Matilla-Peña","doi":"10.1177/17562848231206995","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Transarterial radioembolization (TARE) is increasingly used in patients with hepatocellular carcinoma (HCC). This treatment can induce or impair portal hypertension, leading to hepatic decompensation. TARE also promotes changes in liver and spleen volumes that may modify therapeutic decisions and outcomes after therapy.</p><p><strong>Objectives: </strong>We aimed to investigate the impact of TARE on the incidence of decompensation events and its predictive factors.</p><p><strong>Design: </strong>In all, 63 consecutive patients treated with TARE between February 2012 and December 2018 were retrospectively included.</p><p><strong>Methods: </strong>We assessed clinical (including Barcelona Clinic Liver Cancer stage, portal hypertension assessment, and liver decompensation), laboratory parameters, and liver and spleen volumes before and 6 and 12 weeks after treatment. A multivariate analysis was performed.</p><p><strong>Results: </strong>In total, 18 out of 63 (28.6%) patients had liver decompensation (ascites, variceal bleeding, jaundice, or encephalopathy) within the first 3 months after therapy, not associated with tumor progression. Clinically significant portal hypertension (CSPH) and bilobar treatment independently predicted the development of liver decompensation after TARE. A significant volume increase in the non-treated hemi-liver was observed only in patients with unilobar treatment (median volume increase of 20.2% in patients with right lobe TARE; <i>p</i> = 0.007), especially in those without CSPH. Spleen volume also increased after TARE (median volume increase of 16.1%; <i>p</i> = 0.0001) and was associated with worsening liver function scores and decreased platelet count.</p><p><strong>Conclusion: </strong>Bilobar TARE and CSPH may be associated with an increased risk of liver decompensation in patients with intermediate or advanced HCC. A careful assessment considering these variables before therapy may optimize candidate selection and improve treatment planning.</p>","PeriodicalId":48770,"journal":{"name":"Therapeutic Advances in Gastroenterology","volume":"16 ","pages":"17562848231206995"},"PeriodicalIF":3.4000,"publicationDate":"2023-10-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10619355/pdf/","citationCount":"0","resultStr":"{\"title\":\"Portal hypertension increases the risk of hepatic decompensation after 90Yttrium radioembolization in patients with hepatocellular carcinoma: a cohort study.\",\"authors\":\"Laura Carrión, Ana Clemente-Sánchez, Laura Márquez-Pérez, Javier Orcajo-Rincón, Amanda Rotger, Enrique Ramón-Botella, Manuel González-Leyte, Miguel Echenagusía-Boyra, Arturo Luis Colón, Laura Reguera-Berenguer, Rafael Bañares, Diego Rincón, Ana Matilla-Peña\",\"doi\":\"10.1177/17562848231206995\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Transarterial radioembolization (TARE) is increasingly used in patients with hepatocellular carcinoma (HCC). This treatment can induce or impair portal hypertension, leading to hepatic decompensation. TARE also promotes changes in liver and spleen volumes that may modify therapeutic decisions and outcomes after therapy.</p><p><strong>Objectives: </strong>We aimed to investigate the impact of TARE on the incidence of decompensation events and its predictive factors.</p><p><strong>Design: </strong>In all, 63 consecutive patients treated with TARE between February 2012 and December 2018 were retrospectively included.</p><p><strong>Methods: </strong>We assessed clinical (including Barcelona Clinic Liver Cancer stage, portal hypertension assessment, and liver decompensation), laboratory parameters, and liver and spleen volumes before and 6 and 12 weeks after treatment. A multivariate analysis was performed.</p><p><strong>Results: </strong>In total, 18 out of 63 (28.6%) patients had liver decompensation (ascites, variceal bleeding, jaundice, or encephalopathy) within the first 3 months after therapy, not associated with tumor progression. Clinically significant portal hypertension (CSPH) and bilobar treatment independently predicted the development of liver decompensation after TARE. A significant volume increase in the non-treated hemi-liver was observed only in patients with unilobar treatment (median volume increase of 20.2% in patients with right lobe TARE; <i>p</i> = 0.007), especially in those without CSPH. Spleen volume also increased after TARE (median volume increase of 16.1%; <i>p</i> = 0.0001) and was associated with worsening liver function scores and decreased platelet count.</p><p><strong>Conclusion: </strong>Bilobar TARE and CSPH may be associated with an increased risk of liver decompensation in patients with intermediate or advanced HCC. A careful assessment considering these variables before therapy may optimize candidate selection and improve treatment planning.</p>\",\"PeriodicalId\":48770,\"journal\":{\"name\":\"Therapeutic Advances in Gastroenterology\",\"volume\":\"16 \",\"pages\":\"17562848231206995\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2023-10-31\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10619355/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Therapeutic Advances in Gastroenterology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1177/17562848231206995\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Gastroenterology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/17562848231206995","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Portal hypertension increases the risk of hepatic decompensation after 90Yttrium radioembolization in patients with hepatocellular carcinoma: a cohort study.
Background: Transarterial radioembolization (TARE) is increasingly used in patients with hepatocellular carcinoma (HCC). This treatment can induce or impair portal hypertension, leading to hepatic decompensation. TARE also promotes changes in liver and spleen volumes that may modify therapeutic decisions and outcomes after therapy.
Objectives: We aimed to investigate the impact of TARE on the incidence of decompensation events and its predictive factors.
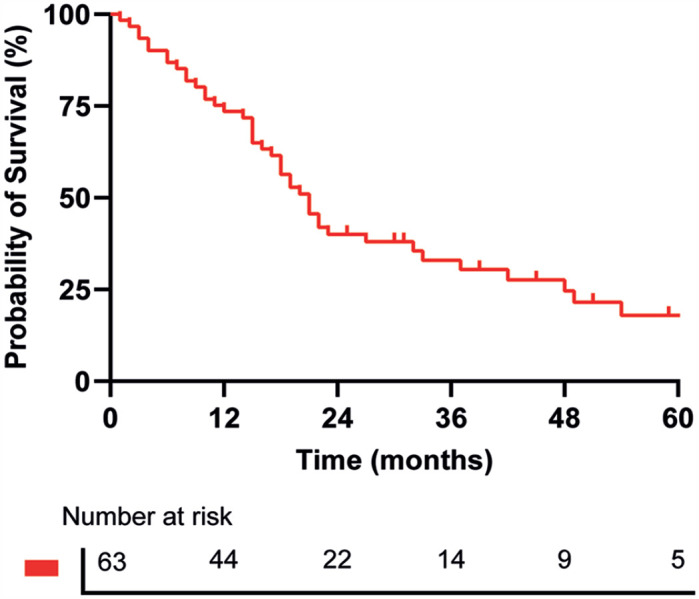
Design: In all, 63 consecutive patients treated with TARE between February 2012 and December 2018 were retrospectively included.
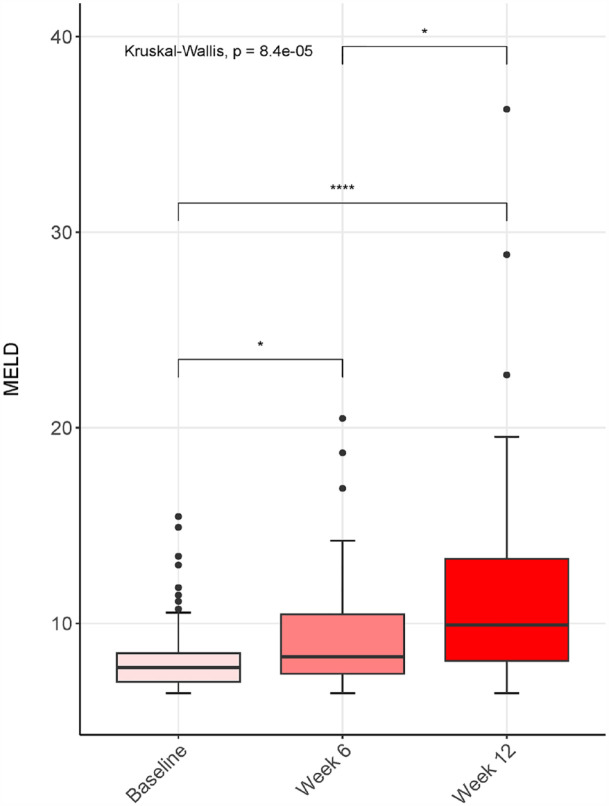
Methods: We assessed clinical (including Barcelona Clinic Liver Cancer stage, portal hypertension assessment, and liver decompensation), laboratory parameters, and liver and spleen volumes before and 6 and 12 weeks after treatment. A multivariate analysis was performed.
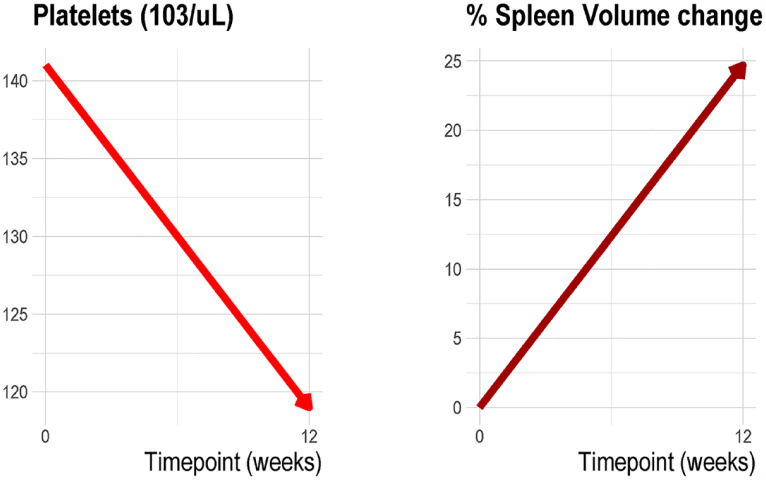
Results: In total, 18 out of 63 (28.6%) patients had liver decompensation (ascites, variceal bleeding, jaundice, or encephalopathy) within the first 3 months after therapy, not associated with tumor progression. Clinically significant portal hypertension (CSPH) and bilobar treatment independently predicted the development of liver decompensation after TARE. A significant volume increase in the non-treated hemi-liver was observed only in patients with unilobar treatment (median volume increase of 20.2% in patients with right lobe TARE; p = 0.007), especially in those without CSPH. Spleen volume also increased after TARE (median volume increase of 16.1%; p = 0.0001) and was associated with worsening liver function scores and decreased platelet count.
Conclusion: Bilobar TARE and CSPH may be associated with an increased risk of liver decompensation in patients with intermediate or advanced HCC. A careful assessment considering these variables before therapy may optimize candidate selection and improve treatment planning.
期刊介绍:
Therapeutic Advances in Gastroenterology is an open access journal which delivers the highest quality peer-reviewed original research articles, reviews, and scholarly comment on pioneering efforts and innovative studies in the medical treatment of gastrointestinal and hepatic disorders. The journal has a strong clinical and pharmacological focus and is aimed at an international audience of clinicians and researchers in gastroenterology and related disciplines, providing an online forum for rapid dissemination of recent research and perspectives in this area.
The editors welcome original research articles across all areas of gastroenterology and hepatology.
The journal publishes original research articles and review articles primarily. Original research manuscripts may include laboratory, animal or human/clinical studies – all phases. Letters to the Editor and Case Reports will also be considered.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
