{"title":"南非一家三级医院因妊娠高血压疾病并发症而入住重症监护病房的患者的预后——一项为期4年的回顾性研究","authors":"S Gama, M Sebitloane, K de Vasconcellos","doi":"10.7196/SAJCC.2019.v35i2.001","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hypertensive disorders of pregnancy (HDP) are a major cause of maternal mortality and adverse outcomes. A previous study in the intensive care unit (ICU) at King Edward VIII Hospital, Durban, South Africa, in 2000 found 10.5% mortality among eclampsia patients.</p><p><strong>Objectives: </strong>To describe the mortality and adverse neurological outcomes associated with HDP in a tertiary ICU, compare these with results from 2000 and describe factors associated therewith.</p><p><strong>Methods: </strong>The data of 85 patients admitted with HDP to ICU at King Edward VIII Hospital from 2010 to 2013 were retrospectively reviewed. Mortality and adverse neurological outcome (Glasgow Coma Scale (GCS) ≤14 on discharge from ICU) were assessed. Two sets of analyses were conducted. The first compared those alive on discharge from ICU with those who died in ICU. The second compared good neurological outcome with poor outcome (adverse neurological outcome, or death).</p><p><strong>Results: </strong>The mortality was 11.6%, and overall, 9% had adverse neurological outcomes. There was no significant difference in mortality between patients with eclampsia in 2010 - 2013 (11.0%) and those in 2000 (10.5%) (p=0.9). Factors associated with mortality were: intra- or postpartum onset of seizures; twins; failure to perform operative delivery when indicated; lowest GCS score <10; failure to use magnesium sulphate when indicated; respiratory failure; and lower respiratory tract infections. Factors associated with poor outcomes (adverse neurological outcome, or death) were: parity (better outcomes in primiparous patients); time of antenatal onset of hypertension (worse if earlier onset); HIV infection; failure to perform operative delivery when indicated; lowest GCS score <10; failure to use magnesium sulphate when indicated; use of anticonvulsants other than magnesium sulphate or benzodiazepines in eclampsia.</p><p><strong>Conclusion: </strong>The lack of improvement in ICU eclampsia mortality demonstrates a need to develop and implement a protocol for HDP management.</p><p><strong>Contributions of the study: </strong>The study provides a comparison of present mortality among eclamptic patients with hyperensive disorders of pregnancy (HDP) with the mortality of eclamptic patients described in an article from the year 2000. It further looks at adverse maternal outcomes, specifically adverse neurological outcomes.In addition, it analyses other factors that may affect outcomes in HDP patients. This information is useful in making recommendations in an attempt to improve the outcomes.</p>","PeriodicalId":75194,"journal":{"name":"The Southern African journal of critical care : the official journal of the Critical Care Society","volume":"35 2","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2019-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.7196/SAJCC.2019.v35i2.001","citationCount":"1","resultStr":"{\"title\":\"Outcomes of patients admitted to the intensive care unit for complications of hypertensive disorders of pregnancy at a South African tertiary hospital - a 4-year retrospective review.\",\"authors\":\"S Gama, M Sebitloane, K de Vasconcellos\",\"doi\":\"10.7196/SAJCC.2019.v35i2.001\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Hypertensive disorders of pregnancy (HDP) are a major cause of maternal mortality and adverse outcomes. A previous study in the intensive care unit (ICU) at King Edward VIII Hospital, Durban, South Africa, in 2000 found 10.5% mortality among eclampsia patients.</p><p><strong>Objectives: </strong>To describe the mortality and adverse neurological outcomes associated with HDP in a tertiary ICU, compare these with results from 2000 and describe factors associated therewith.</p><p><strong>Methods: </strong>The data of 85 patients admitted with HDP to ICU at King Edward VIII Hospital from 2010 to 2013 were retrospectively reviewed. Mortality and adverse neurological outcome (Glasgow Coma Scale (GCS) ≤14 on discharge from ICU) were assessed. Two sets of analyses were conducted. The first compared those alive on discharge from ICU with those who died in ICU. The second compared good neurological outcome with poor outcome (adverse neurological outcome, or death).</p><p><strong>Results: </strong>The mortality was 11.6%, and overall, 9% had adverse neurological outcomes. There was no significant difference in mortality between patients with eclampsia in 2010 - 2013 (11.0%) and those in 2000 (10.5%) (p=0.9). Factors associated with mortality were: intra- or postpartum onset of seizures; twins; failure to perform operative delivery when indicated; lowest GCS score <10; failure to use magnesium sulphate when indicated; respiratory failure; and lower respiratory tract infections. Factors associated with poor outcomes (adverse neurological outcome, or death) were: parity (better outcomes in primiparous patients); time of antenatal onset of hypertension (worse if earlier onset); HIV infection; failure to perform operative delivery when indicated; lowest GCS score <10; failure to use magnesium sulphate when indicated; use of anticonvulsants other than magnesium sulphate or benzodiazepines in eclampsia.</p><p><strong>Conclusion: </strong>The lack of improvement in ICU eclampsia mortality demonstrates a need to develop and implement a protocol for HDP management.</p><p><strong>Contributions of the study: </strong>The study provides a comparison of present mortality among eclamptic patients with hyperensive disorders of pregnancy (HDP) with the mortality of eclamptic patients described in an article from the year 2000. It further looks at adverse maternal outcomes, specifically adverse neurological outcomes.In addition, it analyses other factors that may affect outcomes in HDP patients. This information is useful in making recommendations in an attempt to improve the outcomes.</p>\",\"PeriodicalId\":75194,\"journal\":{\"name\":\"The Southern African journal of critical care : the official journal of the Critical Care Society\",\"volume\":\"35 2\",\"pages\":\"\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2019-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.7196/SAJCC.2019.v35i2.001\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"The Southern African journal of critical care : the official journal of the Critical Care Society\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7196/SAJCC.2019.v35i2.001\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Southern African journal of critical care : the official journal of the Critical Care Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7196/SAJCC.2019.v35i2.001","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Outcomes of patients admitted to the intensive care unit for complications of hypertensive disorders of pregnancy at a South African tertiary hospital - a 4-year retrospective review.
Background: Hypertensive disorders of pregnancy (HDP) are a major cause of maternal mortality and adverse outcomes. A previous study in the intensive care unit (ICU) at King Edward VIII Hospital, Durban, South Africa, in 2000 found 10.5% mortality among eclampsia patients.
Objectives: To describe the mortality and adverse neurological outcomes associated with HDP in a tertiary ICU, compare these with results from 2000 and describe factors associated therewith.
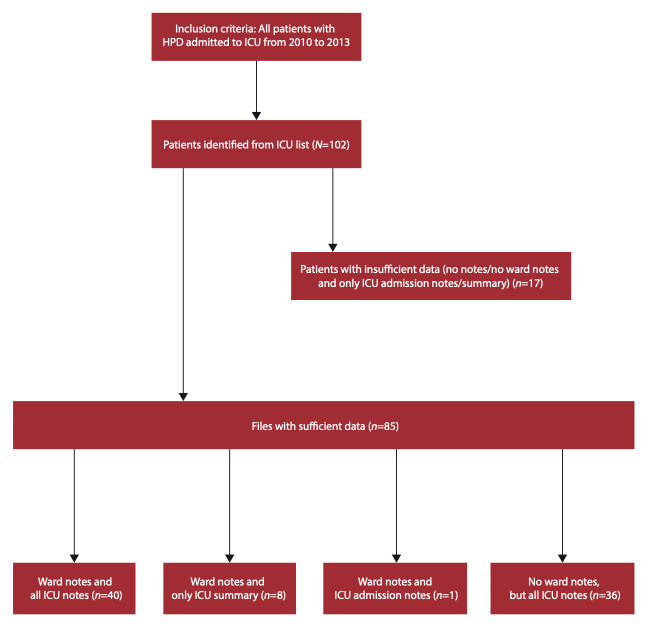
Methods: The data of 85 patients admitted with HDP to ICU at King Edward VIII Hospital from 2010 to 2013 were retrospectively reviewed. Mortality and adverse neurological outcome (Glasgow Coma Scale (GCS) ≤14 on discharge from ICU) were assessed. Two sets of analyses were conducted. The first compared those alive on discharge from ICU with those who died in ICU. The second compared good neurological outcome with poor outcome (adverse neurological outcome, or death).
Results: The mortality was 11.6%, and overall, 9% had adverse neurological outcomes. There was no significant difference in mortality between patients with eclampsia in 2010 - 2013 (11.0%) and those in 2000 (10.5%) (p=0.9). Factors associated with mortality were: intra- or postpartum onset of seizures; twins; failure to perform operative delivery when indicated; lowest GCS score <10; failure to use magnesium sulphate when indicated; respiratory failure; and lower respiratory tract infections. Factors associated with poor outcomes (adverse neurological outcome, or death) were: parity (better outcomes in primiparous patients); time of antenatal onset of hypertension (worse if earlier onset); HIV infection; failure to perform operative delivery when indicated; lowest GCS score <10; failure to use magnesium sulphate when indicated; use of anticonvulsants other than magnesium sulphate or benzodiazepines in eclampsia.
Conclusion: The lack of improvement in ICU eclampsia mortality demonstrates a need to develop and implement a protocol for HDP management.
Contributions of the study: The study provides a comparison of present mortality among eclamptic patients with hyperensive disorders of pregnancy (HDP) with the mortality of eclamptic patients described in an article from the year 2000. It further looks at adverse maternal outcomes, specifically adverse neurological outcomes.In addition, it analyses other factors that may affect outcomes in HDP patients. This information is useful in making recommendations in an attempt to improve the outcomes.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
