Vidhu Anand, Hanwen Hu, Alexander D Weston, Christopher G Scott, Hector I Michelena, Sorin V Pislaru, Rickey E Carter, Patricia A Pellikka
{"title":"基于机器学习的严重主动脉反流患者死亡率风险分层。","authors":"Vidhu Anand, Hanwen Hu, Alexander D Weston, Christopher G Scott, Hector I Michelena, Sorin V Pislaru, Rickey E Carter, Patricia A Pellikka","doi":"10.1093/ehjdh/ztad006","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The current guidelines recommend aortic valve intervention in patients with severe aortic regurgitation (AR) with the onset of symptoms, left ventricular enlargement, or systolic dysfunction. Recent studies have suggested that we might be missing the window of early intervention in a significant number of patients by following the guidelines.</p><p><strong>Methods and results: </strong>The overarching goal was to determine if machine learning (ML)-based algorithms could be trained to identify patients at risk for death from AR independent of aortic valve replacement (AVR). Models were trained with five-fold cross-validation on a dataset of 1035 patients, and performance was reported on an independent dataset of 207 patients. Optimal predictive performance was observed with a conditional random survival forest model. A subset of 19/41 variables was selected for inclusion in the final model. Variable selection was performed with 10-fold cross-validation using random survival forest model. The top variables included were age, body surface area, body mass index, diastolic blood pressure, New York Heart Association class, AVR, comorbidities, ejection fraction, end-diastolic volume, and end-systolic dimension, and the relative variable importance averaged across five splits of cross-validation in each repeat were evaluated. The concordance index for predicting survival of the best-performing model was 0.84 at 1 year, 0.86 at 2 years, and 0.87 overall, respectively.</p><p><strong>Conclusion: </strong>Using common echocardiographic parameters and patient characteristics, we successfully trained multiple ML models to predict survival in patients with severe AR. This technique could be applied to identify high-risk patients who would benefit from early intervention, thereby improving patient outcomes.</p>","PeriodicalId":72965,"journal":{"name":"European heart journal. Digital health","volume":"4 3","pages":"188-195"},"PeriodicalIF":4.4000,"publicationDate":"2023-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/41/f5/ztad006.PMC10232267.pdf","citationCount":"1","resultStr":"{\"title\":\"Machine learning-based risk stratification for mortality in patients with severe aortic regurgitation.\",\"authors\":\"Vidhu Anand, Hanwen Hu, Alexander D Weston, Christopher G Scott, Hector I Michelena, Sorin V Pislaru, Rickey E Carter, Patricia A Pellikka\",\"doi\":\"10.1093/ehjdh/ztad006\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>The current guidelines recommend aortic valve intervention in patients with severe aortic regurgitation (AR) with the onset of symptoms, left ventricular enlargement, or systolic dysfunction. Recent studies have suggested that we might be missing the window of early intervention in a significant number of patients by following the guidelines.</p><p><strong>Methods and results: </strong>The overarching goal was to determine if machine learning (ML)-based algorithms could be trained to identify patients at risk for death from AR independent of aortic valve replacement (AVR). Models were trained with five-fold cross-validation on a dataset of 1035 patients, and performance was reported on an independent dataset of 207 patients. Optimal predictive performance was observed with a conditional random survival forest model. A subset of 19/41 variables was selected for inclusion in the final model. Variable selection was performed with 10-fold cross-validation using random survival forest model. The top variables included were age, body surface area, body mass index, diastolic blood pressure, New York Heart Association class, AVR, comorbidities, ejection fraction, end-diastolic volume, and end-systolic dimension, and the relative variable importance averaged across five splits of cross-validation in each repeat were evaluated. The concordance index for predicting survival of the best-performing model was 0.84 at 1 year, 0.86 at 2 years, and 0.87 overall, respectively.</p><p><strong>Conclusion: </strong>Using common echocardiographic parameters and patient characteristics, we successfully trained multiple ML models to predict survival in patients with severe AR. This technique could be applied to identify high-risk patients who would benefit from early intervention, thereby improving patient outcomes.</p>\",\"PeriodicalId\":72965,\"journal\":{\"name\":\"European heart journal. Digital health\",\"volume\":\"4 3\",\"pages\":\"188-195\"},\"PeriodicalIF\":4.4000,\"publicationDate\":\"2023-05-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/41/f5/ztad006.PMC10232267.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European heart journal. Digital health\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjdh/ztad006\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European heart journal. Digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/ehjdh/ztad006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Machine learning-based risk stratification for mortality in patients with severe aortic regurgitation.
Aims: The current guidelines recommend aortic valve intervention in patients with severe aortic regurgitation (AR) with the onset of symptoms, left ventricular enlargement, or systolic dysfunction. Recent studies have suggested that we might be missing the window of early intervention in a significant number of patients by following the guidelines.
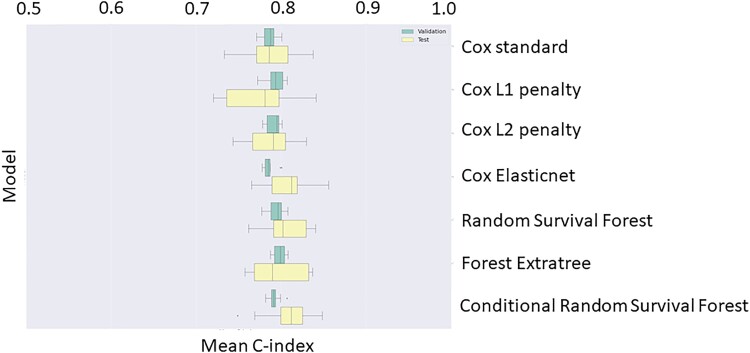
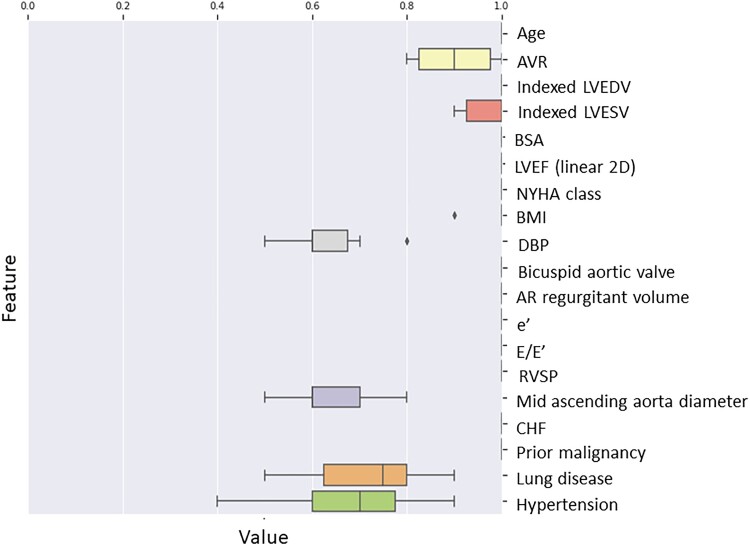
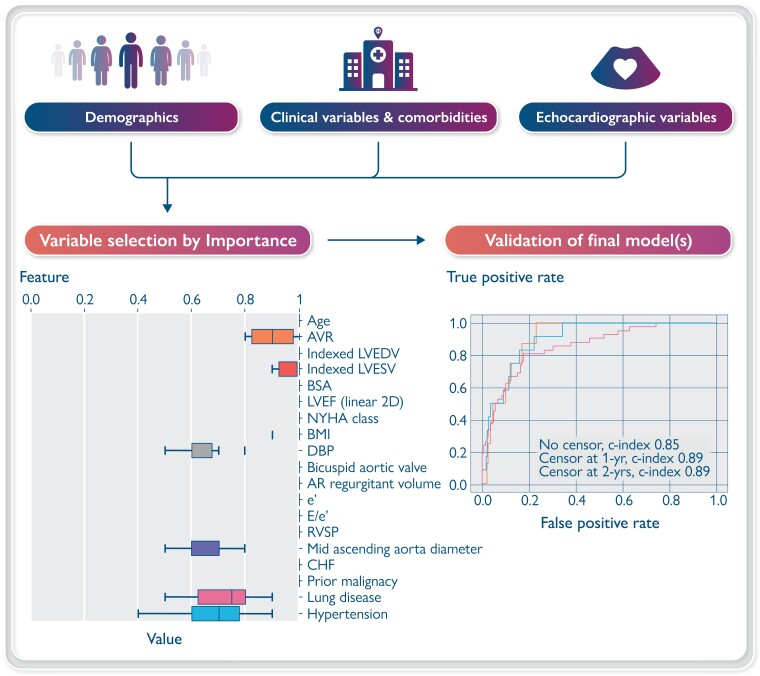
Methods and results: The overarching goal was to determine if machine learning (ML)-based algorithms could be trained to identify patients at risk for death from AR independent of aortic valve replacement (AVR). Models were trained with five-fold cross-validation on a dataset of 1035 patients, and performance was reported on an independent dataset of 207 patients. Optimal predictive performance was observed with a conditional random survival forest model. A subset of 19/41 variables was selected for inclusion in the final model. Variable selection was performed with 10-fold cross-validation using random survival forest model. The top variables included were age, body surface area, body mass index, diastolic blood pressure, New York Heart Association class, AVR, comorbidities, ejection fraction, end-diastolic volume, and end-systolic dimension, and the relative variable importance averaged across five splits of cross-validation in each repeat were evaluated. The concordance index for predicting survival of the best-performing model was 0.84 at 1 year, 0.86 at 2 years, and 0.87 overall, respectively.
Conclusion: Using common echocardiographic parameters and patient characteristics, we successfully trained multiple ML models to predict survival in patients with severe AR. This technique could be applied to identify high-risk patients who would benefit from early intervention, thereby improving patient outcomes.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
