Benjamin C Park, Sathya Narayanan, Alexander Gavraldis, Fei Ye, Run Fan, Ryan J Sullivan, Genevieve Boland, Kerry L Reynolds, Justin M Balko, Matteo S Carlino, Georgina V Long, Leyre Zubiri, Alexander M Menzies, Douglas B Johnson
{"title":"黑色素瘤患者中罕见的免疫相关不良事件:发生率、范围和临床表现。","authors":"Benjamin C Park, Sathya Narayanan, Alexander Gavraldis, Fei Ye, Run Fan, Ryan J Sullivan, Genevieve Boland, Kerry L Reynolds, Justin M Balko, Matteo S Carlino, Georgina V Long, Leyre Zubiri, Alexander M Menzies, Douglas B Johnson","doi":"10.1080/2162402X.2023.2188719","DOIUrl":null,"url":null,"abstract":"<p><p>Immune-related adverse events (irAEs) are side effects of immune checkpoint inhibitor therapy (ICI). While common irAEs have been well characterized, there are more limited data on rare immune related adverse events (RirAEs) due to low incidence. Lack of characterization of these entities has led to difficulties in accurate diagnosis and management. Here, we conducted a multi-institution analysis of all patients with stage III/IV melanoma who developed RirAEs after being treated with ICIs (anti-PD-1/L1, anti-CTLA-4, and combination PD-1/CTLA-4 blockade) at three institutions (Vanderbilt University Medical Center, Massachusetts General Hospital, and Melanoma Institute of Australia). RirAEs were defined as those occurring in approximately <1% of patients treated with anti-PD-1 or <2% with combination. Of 2834 patients who received ICIs, 82 developed RirAEs and were more common with combination PD-1/CTLA-4 blockade (4.6%) vs. anti-PD-1/L1 agents (2.8%). Overall median time from ICI start to RirAE was 86 days (interquartile range 42-235 days) with significantly earlier onset in combination therapy (<i>p</i> < 0.001). The spectrum of RirAEs spanned across several organ systems. Most RirAEs were grade 2 (57 [41.3%]) and grade 3 (40 [29.0%]) with relatively few grade 4 (11 [8.0%]) or 5 (5 [3.6%]) events. Steroid re-escalation (21.4%) or additional immunosuppression (13.8%) were commonly required. RirAE recurrence occurred in 22.6% with ICI rechallenge; 37.1% had new irAEs with rechallenge. In conclusion, RirAEs associated with ICIs in melanoma patients occurred, in aggregate, in 2-5% of patients treated with anti-PD-1-based therapy. Steroid re-escalation and alternative immunosuppression use were frequently required but fatal irAEs were fairly uncommon.</p>","PeriodicalId":19683,"journal":{"name":"Oncoimmunology","volume":"12 1","pages":"2188719"},"PeriodicalIF":7.2000,"publicationDate":"2023-03-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/15/f7/KONI_12_2188719.PMC10012911.pdf","citationCount":"0","resultStr":"{\"title\":\"Rare immune-related adverse events in patients with melanoma: incidence, spectrum, and clinical presentations.\",\"authors\":\"Benjamin C Park, Sathya Narayanan, Alexander Gavraldis, Fei Ye, Run Fan, Ryan J Sullivan, Genevieve Boland, Kerry L Reynolds, Justin M Balko, Matteo S Carlino, Georgina V Long, Leyre Zubiri, Alexander M Menzies, Douglas B Johnson\",\"doi\":\"10.1080/2162402X.2023.2188719\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Immune-related adverse events (irAEs) are side effects of immune checkpoint inhibitor therapy (ICI). While common irAEs have been well characterized, there are more limited data on rare immune related adverse events (RirAEs) due to low incidence. Lack of characterization of these entities has led to difficulties in accurate diagnosis and management. Here, we conducted a multi-institution analysis of all patients with stage III/IV melanoma who developed RirAEs after being treated with ICIs (anti-PD-1/L1, anti-CTLA-4, and combination PD-1/CTLA-4 blockade) at three institutions (Vanderbilt University Medical Center, Massachusetts General Hospital, and Melanoma Institute of Australia). RirAEs were defined as those occurring in approximately <1% of patients treated with anti-PD-1 or <2% with combination. Of 2834 patients who received ICIs, 82 developed RirAEs and were more common with combination PD-1/CTLA-4 blockade (4.6%) vs. anti-PD-1/L1 agents (2.8%). Overall median time from ICI start to RirAE was 86 days (interquartile range 42-235 days) with significantly earlier onset in combination therapy (<i>p</i> < 0.001). The spectrum of RirAEs spanned across several organ systems. Most RirAEs were grade 2 (57 [41.3%]) and grade 3 (40 [29.0%]) with relatively few grade 4 (11 [8.0%]) or 5 (5 [3.6%]) events. Steroid re-escalation (21.4%) or additional immunosuppression (13.8%) were commonly required. RirAE recurrence occurred in 22.6% with ICI rechallenge; 37.1% had new irAEs with rechallenge. In conclusion, RirAEs associated with ICIs in melanoma patients occurred, in aggregate, in 2-5% of patients treated with anti-PD-1-based therapy. Steroid re-escalation and alternative immunosuppression use were frequently required but fatal irAEs were fairly uncommon.</p>\",\"PeriodicalId\":19683,\"journal\":{\"name\":\"Oncoimmunology\",\"volume\":\"12 1\",\"pages\":\"2188719\"},\"PeriodicalIF\":7.2000,\"publicationDate\":\"2023-03-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/15/f7/KONI_12_2188719.PMC10012911.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Oncoimmunology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1080/2162402X.2023.2188719\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2023/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Oncoimmunology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1080/2162402X.2023.2188719","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2023/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Rare immune-related adverse events in patients with melanoma: incidence, spectrum, and clinical presentations.
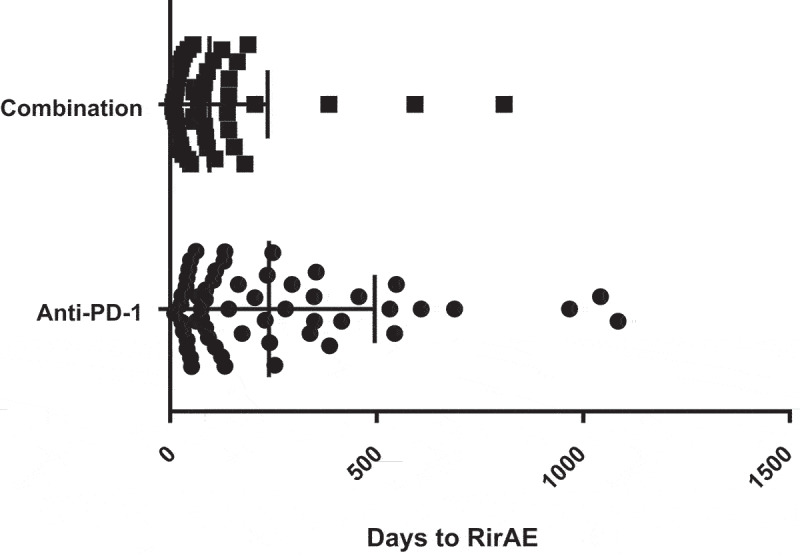
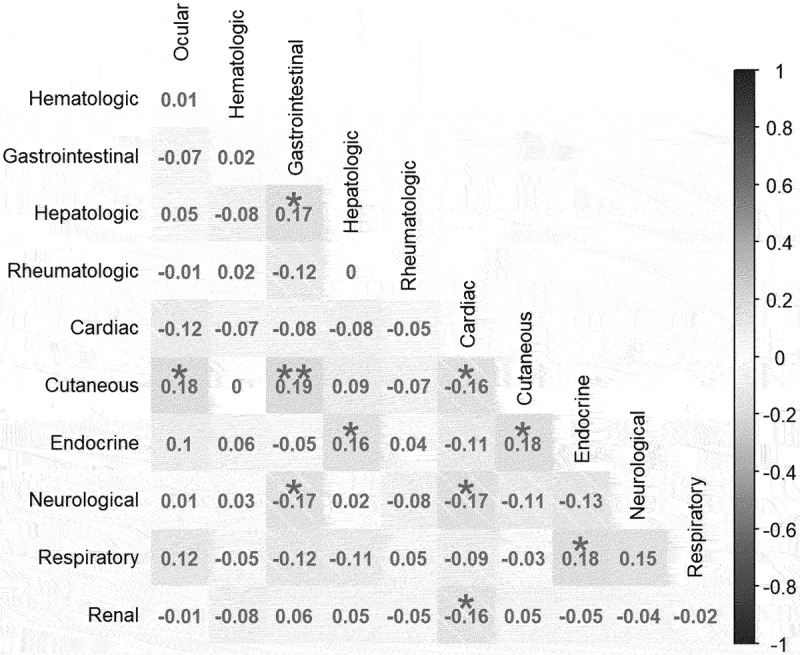
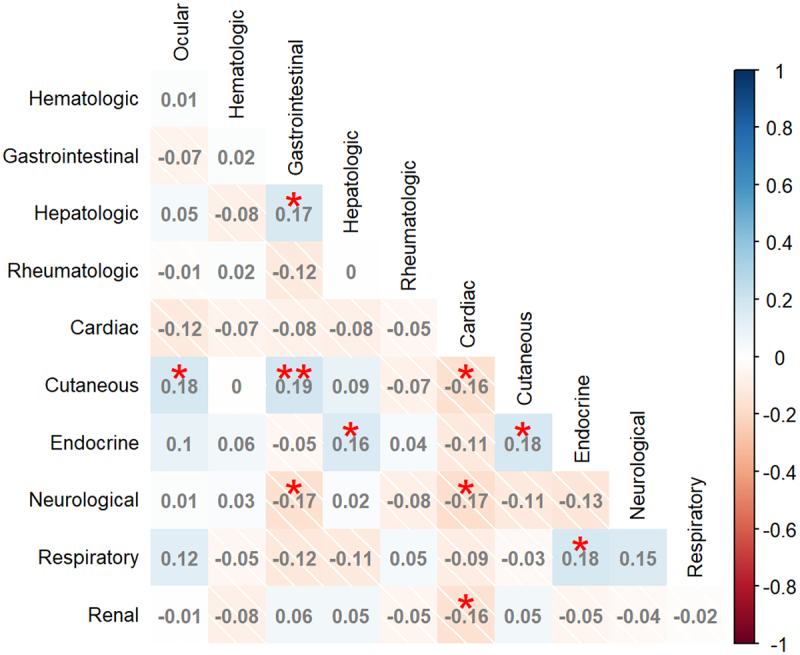
Immune-related adverse events (irAEs) are side effects of immune checkpoint inhibitor therapy (ICI). While common irAEs have been well characterized, there are more limited data on rare immune related adverse events (RirAEs) due to low incidence. Lack of characterization of these entities has led to difficulties in accurate diagnosis and management. Here, we conducted a multi-institution analysis of all patients with stage III/IV melanoma who developed RirAEs after being treated with ICIs (anti-PD-1/L1, anti-CTLA-4, and combination PD-1/CTLA-4 blockade) at three institutions (Vanderbilt University Medical Center, Massachusetts General Hospital, and Melanoma Institute of Australia). RirAEs were defined as those occurring in approximately <1% of patients treated with anti-PD-1 or <2% with combination. Of 2834 patients who received ICIs, 82 developed RirAEs and were more common with combination PD-1/CTLA-4 blockade (4.6%) vs. anti-PD-1/L1 agents (2.8%). Overall median time from ICI start to RirAE was 86 days (interquartile range 42-235 days) with significantly earlier onset in combination therapy (p < 0.001). The spectrum of RirAEs spanned across several organ systems. Most RirAEs were grade 2 (57 [41.3%]) and grade 3 (40 [29.0%]) with relatively few grade 4 (11 [8.0%]) or 5 (5 [3.6%]) events. Steroid re-escalation (21.4%) or additional immunosuppression (13.8%) were commonly required. RirAE recurrence occurred in 22.6% with ICI rechallenge; 37.1% had new irAEs with rechallenge. In conclusion, RirAEs associated with ICIs in melanoma patients occurred, in aggregate, in 2-5% of patients treated with anti-PD-1-based therapy. Steroid re-escalation and alternative immunosuppression use were frequently required but fatal irAEs were fairly uncommon.
期刊介绍:
Tumor immunology explores the natural and therapy-induced recognition of cancers, along with the complex interplay between oncogenesis, inflammation, and immunosurveillance. In response to recent advancements, a new journal, OncoImmunology, is being launched to specifically address tumor immunology. The field has seen significant progress with the clinical demonstration and FDA approval of anticancer immunotherapies. There's also growing evidence suggesting that many current chemotherapeutic agents rely on immune effectors for their efficacy.
While oncologists have historically utilized chemotherapeutic and radiotherapeutic regimens successfully, they may have unwittingly leveraged the immune system's ability to recognize tumor-specific antigens and control cancer growth. Consequently, immunological biomarkers are increasingly crucial for cancer prognosis and predicting chemotherapy efficacy. There's strong support for combining conventional anticancer therapies with immunotherapies. OncoImmunology will welcome high-profile submissions spanning fundamental, translational, and clinical aspects of tumor immunology, including solid and hematological cancers, inflammation, and both innate and acquired immune responses.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
