{"title":"一种罕见的急性胸主动脉夹层表现。","authors":"MacKenzie Barton, Hao Wang","doi":"10.14740/jocmr4921","DOIUrl":null,"url":null,"abstract":"<p><p>We present a case of a 40-year-old Caucasian male with past medical history of polysubstance abuse (cocaine and methamphetamine), who presented to the emergency department (ED) complaining of intermittent cough with associated chest discomfort and shortness of breath for 2 weeks. Initial vital signs demonstrated borderline tachycardia (98 beats per minute), tachypnea (37 times per minutes), and hypoxia (oxygen saturation 89% on room air), and his physical exam was grossly unremarkable. A preliminary workup including a computed tomography angiography (CTA) revealed a type A aortic dissection with both thoracic and abdominal involvement for which the patient was admitted. This patient had resection of the ascending aorta with graft placement, cardiopulmonary bypass, aortic root replacement using composite prosthesis and left and right coronary reconstruction and reimplantation and survived a complicated hospital course. This case demonstrates the classic association known to exist between recreational drug use, specifically stimulants such as cocaine and amphetamines, and acute aortic dissection (AAD). However, such a presentation of borderline subacute, painless dissection in the setting of polysubstance use raises further questions, since uncommon AAD is typically found in higher-risk populations such as those with connective tissue disorders (Marfan syndrome, Ehlers-Danlos syndrome, Loeys-Dietz syndrome), bicuspid aortic valve, chronic hypertension, or previous aortic pathology. We therefore suggest clinicians strongly consider uncommon AAD as part of their differential diagnosis in patients with known or highly suspected polysubstance abuse.</p>","PeriodicalId":15431,"journal":{"name":"Journal of Clinical Medicine Research","volume":"15 6","pages":"332-335"},"PeriodicalIF":0.0000,"publicationDate":"2023-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f0/12/jocmr-15-332.PMC10332876.pdf","citationCount":"1","resultStr":"{\"title\":\"An Uncommon Presentation of Acute Thoracic Aortic Dissection.\",\"authors\":\"MacKenzie Barton, Hao Wang\",\"doi\":\"10.14740/jocmr4921\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>We present a case of a 40-year-old Caucasian male with past medical history of polysubstance abuse (cocaine and methamphetamine), who presented to the emergency department (ED) complaining of intermittent cough with associated chest discomfort and shortness of breath for 2 weeks. Initial vital signs demonstrated borderline tachycardia (98 beats per minute), tachypnea (37 times per minutes), and hypoxia (oxygen saturation 89% on room air), and his physical exam was grossly unremarkable. A preliminary workup including a computed tomography angiography (CTA) revealed a type A aortic dissection with both thoracic and abdominal involvement for which the patient was admitted. This patient had resection of the ascending aorta with graft placement, cardiopulmonary bypass, aortic root replacement using composite prosthesis and left and right coronary reconstruction and reimplantation and survived a complicated hospital course. This case demonstrates the classic association known to exist between recreational drug use, specifically stimulants such as cocaine and amphetamines, and acute aortic dissection (AAD). However, such a presentation of borderline subacute, painless dissection in the setting of polysubstance use raises further questions, since uncommon AAD is typically found in higher-risk populations such as those with connective tissue disorders (Marfan syndrome, Ehlers-Danlos syndrome, Loeys-Dietz syndrome), bicuspid aortic valve, chronic hypertension, or previous aortic pathology. We therefore suggest clinicians strongly consider uncommon AAD as part of their differential diagnosis in patients with known or highly suspected polysubstance abuse.</p>\",\"PeriodicalId\":15431,\"journal\":{\"name\":\"Journal of Clinical Medicine Research\",\"volume\":\"15 6\",\"pages\":\"332-335\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2023-06-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f0/12/jocmr-15-332.PMC10332876.pdf\",\"citationCount\":\"1\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Clinical Medicine Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14740/jocmr4921\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Medicine Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/jocmr4921","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
An Uncommon Presentation of Acute Thoracic Aortic Dissection.
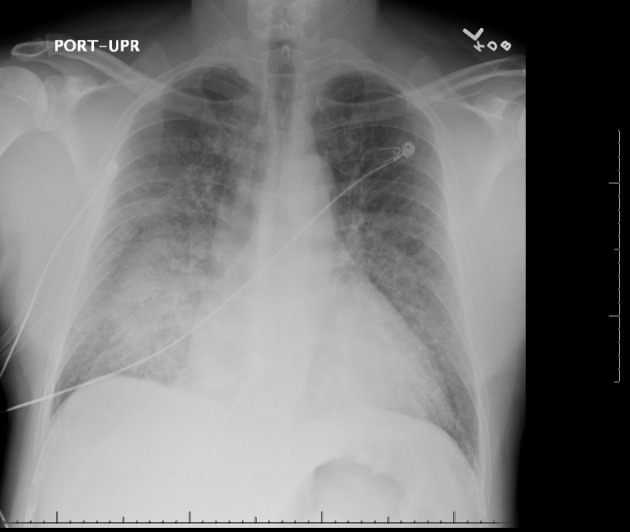
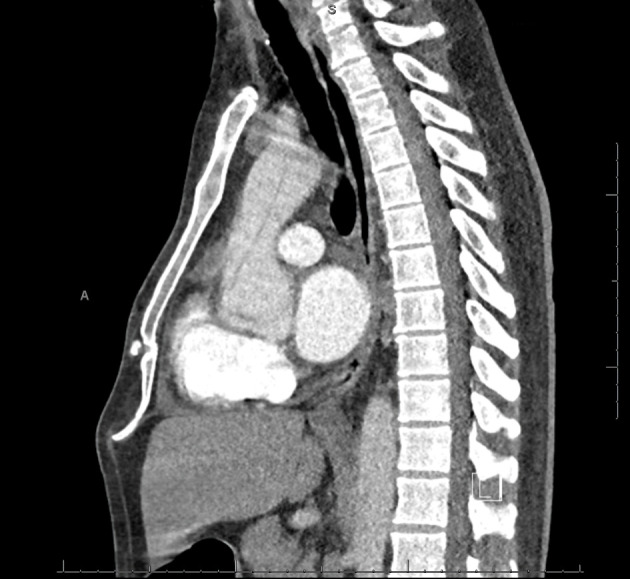
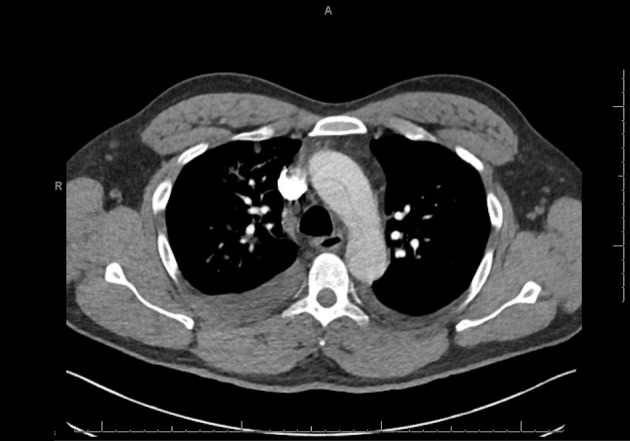
We present a case of a 40-year-old Caucasian male with past medical history of polysubstance abuse (cocaine and methamphetamine), who presented to the emergency department (ED) complaining of intermittent cough with associated chest discomfort and shortness of breath for 2 weeks. Initial vital signs demonstrated borderline tachycardia (98 beats per minute), tachypnea (37 times per minutes), and hypoxia (oxygen saturation 89% on room air), and his physical exam was grossly unremarkable. A preliminary workup including a computed tomography angiography (CTA) revealed a type A aortic dissection with both thoracic and abdominal involvement for which the patient was admitted. This patient had resection of the ascending aorta with graft placement, cardiopulmonary bypass, aortic root replacement using composite prosthesis and left and right coronary reconstruction and reimplantation and survived a complicated hospital course. This case demonstrates the classic association known to exist between recreational drug use, specifically stimulants such as cocaine and amphetamines, and acute aortic dissection (AAD). However, such a presentation of borderline subacute, painless dissection in the setting of polysubstance use raises further questions, since uncommon AAD is typically found in higher-risk populations such as those with connective tissue disorders (Marfan syndrome, Ehlers-Danlos syndrome, Loeys-Dietz syndrome), bicuspid aortic valve, chronic hypertension, or previous aortic pathology. We therefore suggest clinicians strongly consider uncommon AAD as part of their differential diagnosis in patients with known or highly suspected polysubstance abuse.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
