Anders Damgaard Møller Schlünsen, David Høyrup Christiansen, Ulrich Fredberg, Peter Vedsted
{"title":"24小时门诊对医院门诊随访中慢性病患者的有效性:一项基于登记的医疗保健利用和死亡率的对照队列研究","authors":"Anders Damgaard Møller Schlünsen, David Høyrup Christiansen, Ulrich Fredberg, Peter Vedsted","doi":"10.1136/ihj-2020-000069","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To evaluate the effectiveness of a 24-hour telephone access outpatient clinic (24-hour access clinic) in terms of healthcare utilisation and mortality in patients with five chronic conditions (chronic obstructive pulmonary disease, atrial fibrillation/flutter, congestive heart failure, inflammatory bowel disease and chronic liver disease).</p><p><strong>Methods and analysis: </strong>This was a registry-based controlled cohort study. The 24-hour access clinic was established at Silkeborg Regional Hospital in Central Denmark Region. The five other regional hospitals served as comparison hospitals. The 24-hour access clinic allowed patients with five chronic conditions with ongoing hospital outpatient follow-up to call the hospital outpatient clinic in case of an exacerbation. Outcomes were use of hospital admissions, length of stay (LOS), outpatient visits, contacts to general practice and all-cause mortality during 18 months of follow-up.</p><p><strong>Results: </strong>The study included 992 the 24-hour access patients and 3878 usual care patients. For the five conditions combined, the 24 hours access patients had fewer all-cause admissions (incidence rate ratio (IRR) 0.81, 95% Cl 0.71 to 0.92), general practice out-of-hours contacts (IRR 0.81, 95% C 0.71 to.92) and shorter LOS (IRR 0.71, 95% CI 0.57 to 0.88). The rate of all-cause outpatient visits tended to be higher (IRR 1.07, 95% CI 0.99 to 1.15). General practice daytime contacts were similar between the groups, and there was no significant difference in mortality.</p><p><strong>Conclusions: </strong>The results suggest that a 24-hour telephone access clinic may lead to enhanced integration of care measured as unplanned acute care substituted with planned outpatient care.</p>","PeriodicalId":73393,"journal":{"name":"Integrated healthcare journal","volume":"4 1","pages":"e000069"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4e/d9/ihj-2020-000069.PMC10241022.pdf","citationCount":"0","resultStr":"{\"title\":\"Effectiveness of a 24-hour access outpatient clinic for patients with chronic conditions in hospital outpatient follow-up: a registry-based controlled cohort study of healthcare utilisation and mortality.\",\"authors\":\"Anders Damgaard Møller Schlünsen, David Høyrup Christiansen, Ulrich Fredberg, Peter Vedsted\",\"doi\":\"10.1136/ihj-2020-000069\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To evaluate the effectiveness of a 24-hour telephone access outpatient clinic (24-hour access clinic) in terms of healthcare utilisation and mortality in patients with five chronic conditions (chronic obstructive pulmonary disease, atrial fibrillation/flutter, congestive heart failure, inflammatory bowel disease and chronic liver disease).</p><p><strong>Methods and analysis: </strong>This was a registry-based controlled cohort study. The 24-hour access clinic was established at Silkeborg Regional Hospital in Central Denmark Region. The five other regional hospitals served as comparison hospitals. The 24-hour access clinic allowed patients with five chronic conditions with ongoing hospital outpatient follow-up to call the hospital outpatient clinic in case of an exacerbation. Outcomes were use of hospital admissions, length of stay (LOS), outpatient visits, contacts to general practice and all-cause mortality during 18 months of follow-up.</p><p><strong>Results: </strong>The study included 992 the 24-hour access patients and 3878 usual care patients. For the five conditions combined, the 24 hours access patients had fewer all-cause admissions (incidence rate ratio (IRR) 0.81, 95% Cl 0.71 to 0.92), general practice out-of-hours contacts (IRR 0.81, 95% C 0.71 to.92) and shorter LOS (IRR 0.71, 95% CI 0.57 to 0.88). The rate of all-cause outpatient visits tended to be higher (IRR 1.07, 95% CI 0.99 to 1.15). General practice daytime contacts were similar between the groups, and there was no significant difference in mortality.</p><p><strong>Conclusions: </strong>The results suggest that a 24-hour telephone access clinic may lead to enhanced integration of care measured as unplanned acute care substituted with planned outpatient care.</p>\",\"PeriodicalId\":73393,\"journal\":{\"name\":\"Integrated healthcare journal\",\"volume\":\"4 1\",\"pages\":\"e000069\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2022-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/4e/d9/ihj-2020-000069.PMC10241022.pdf\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Integrated healthcare journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/ihj-2020-000069\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Integrated healthcare journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/ihj-2020-000069","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
目的:评价24小时电话门诊(24小时门诊)在五种慢性病(慢性阻塞性肺病、心房颤动/扑动、充血性心力衰竭、炎症性肠病和慢性肝病)患者的保健利用和死亡率方面的有效性。方法和分析:这是一项基于登记的对照队列研究。在丹麦中部地区的西尔克堡地区医院设立了24小时门诊。其他5家区域医院作为比较医院。24小时门诊允许患有五种慢性疾病并接受医院门诊随访的患者在病情加重时致电医院门诊。结果是18个月随访期间住院次数、住院时间(LOS)、门诊次数、全科就诊和全因死亡率。结果:纳入24小时就诊患者992例,常规护理患者3878例。对于这五种情况,24小时就诊患者的全因入院率(发病率比(IRR) 0.81, 95% Cl 0.71至0.92)、全科门诊非工作时间接触(IRR 0.81, 95% CI 0.71至0.92)和较短的LOS (IRR 0.71, 95% CI 0.57至0.88)较少。全因门诊就诊率趋于较高(IRR 1.07, 95% CI 0.99 ~ 1.15)。两组之间白天的常规接触相似,死亡率无显著差异。结论:结果表明,一个24小时电话访问诊所可能会导致加强整合的护理测量为计划外的急性护理取代计划门诊护理。
Effectiveness of a 24-hour access outpatient clinic for patients with chronic conditions in hospital outpatient follow-up: a registry-based controlled cohort study of healthcare utilisation and mortality.
Objective: To evaluate the effectiveness of a 24-hour telephone access outpatient clinic (24-hour access clinic) in terms of healthcare utilisation and mortality in patients with five chronic conditions (chronic obstructive pulmonary disease, atrial fibrillation/flutter, congestive heart failure, inflammatory bowel disease and chronic liver disease).
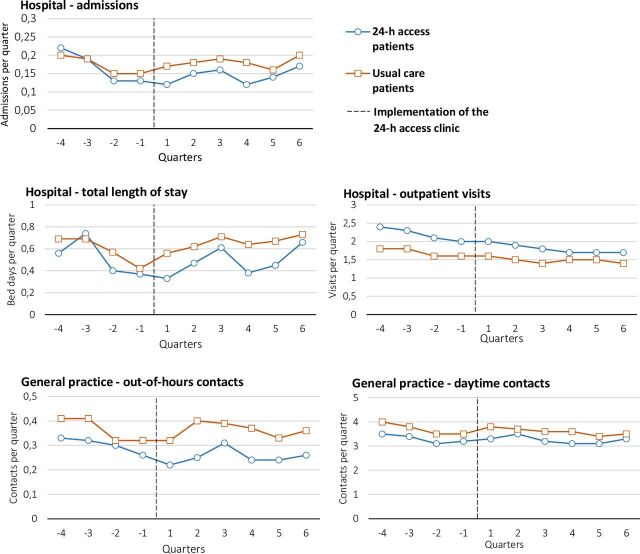
Methods and analysis: This was a registry-based controlled cohort study. The 24-hour access clinic was established at Silkeborg Regional Hospital in Central Denmark Region. The five other regional hospitals served as comparison hospitals. The 24-hour access clinic allowed patients with five chronic conditions with ongoing hospital outpatient follow-up to call the hospital outpatient clinic in case of an exacerbation. Outcomes were use of hospital admissions, length of stay (LOS), outpatient visits, contacts to general practice and all-cause mortality during 18 months of follow-up.
Results: The study included 992 the 24-hour access patients and 3878 usual care patients. For the five conditions combined, the 24 hours access patients had fewer all-cause admissions (incidence rate ratio (IRR) 0.81, 95% Cl 0.71 to 0.92), general practice out-of-hours contacts (IRR 0.81, 95% C 0.71 to.92) and shorter LOS (IRR 0.71, 95% CI 0.57 to 0.88). The rate of all-cause outpatient visits tended to be higher (IRR 1.07, 95% CI 0.99 to 1.15). General practice daytime contacts were similar between the groups, and there was no significant difference in mortality.
Conclusions: The results suggest that a 24-hour telephone access clinic may lead to enhanced integration of care measured as unplanned acute care substituted with planned outpatient care.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
