Kathryn Bullen, Nicola Hall, John Sherwood, Nicola Wake, Gemma Donovan
{"title":"初级保健处方错误报告:叙述综合系统回顾。","authors":"Kathryn Bullen, Nicola Hall, John Sherwood, Nicola Wake, Gemma Donovan","doi":"10.1136/ihj-2019-000026","DOIUrl":null,"url":null,"abstract":"<p><p>Prescribing errors can cause avoidable harm to patients. Most prescriptions originate in primary care, where medications tend to be self-administered and errors have the most potential to cause harm. Reporting prescribing errors can identify trends and reduce the risk of the reoccurrence of incidents; however, under-reporting is common. The organisation of care and the movement of prescriptions from general practice to community pharmacy may create difficulties for professionals to effectively report errors. This review aims specifically to identify primary research studies that examine barriers and facilitators to prescription error reporting across primary care. A systematic research of the literature was completed in July 2019. Four databases (PubMed/Medline, Cochrane, CINAHL and Web of Science) were searched for relevant studies. No date or language limits were applied. Eligible studies were critically appraised using the Mixed Methods Appraisal Tool, and data were descriptively and narratively synthesised. Ten articles were included in the final analysis. Seven studies considered prescription errors and error reporting within general practice and three within a community pharmacy setting. Findings from the included studies are presented across five themes, including definition of an error, prescribing error reporting culture, reporting processes, communication and capacity. Healthcare professionals appreciate the value of prescription error reporting, but there are key barriers to implementation, including time, fear of reprisal and organisation separation within primary care.</p>","PeriodicalId":73393,"journal":{"name":"Integrated healthcare journal","volume":"2 1","pages":"e000026"},"PeriodicalIF":0.0000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1136/ihj-2019-000026","citationCount":"4","resultStr":"{\"title\":\"Prescribing error reporting in primary care: a narrative synthesis systematic review.\",\"authors\":\"Kathryn Bullen, Nicola Hall, John Sherwood, Nicola Wake, Gemma Donovan\",\"doi\":\"10.1136/ihj-2019-000026\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Prescribing errors can cause avoidable harm to patients. Most prescriptions originate in primary care, where medications tend to be self-administered and errors have the most potential to cause harm. Reporting prescribing errors can identify trends and reduce the risk of the reoccurrence of incidents; however, under-reporting is common. The organisation of care and the movement of prescriptions from general practice to community pharmacy may create difficulties for professionals to effectively report errors. This review aims specifically to identify primary research studies that examine barriers and facilitators to prescription error reporting across primary care. A systematic research of the literature was completed in July 2019. Four databases (PubMed/Medline, Cochrane, CINAHL and Web of Science) were searched for relevant studies. No date or language limits were applied. Eligible studies were critically appraised using the Mixed Methods Appraisal Tool, and data were descriptively and narratively synthesised. Ten articles were included in the final analysis. Seven studies considered prescription errors and error reporting within general practice and three within a community pharmacy setting. Findings from the included studies are presented across five themes, including definition of an error, prescribing error reporting culture, reporting processes, communication and capacity. Healthcare professionals appreciate the value of prescription error reporting, but there are key barriers to implementation, including time, fear of reprisal and organisation separation within primary care.</p>\",\"PeriodicalId\":73393,\"journal\":{\"name\":\"Integrated healthcare journal\",\"volume\":\"2 1\",\"pages\":\"e000026\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2020-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1136/ihj-2019-000026\",\"citationCount\":\"4\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Integrated healthcare journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1136/ihj-2019-000026\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Integrated healthcare journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/ihj-2019-000026","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 4
摘要
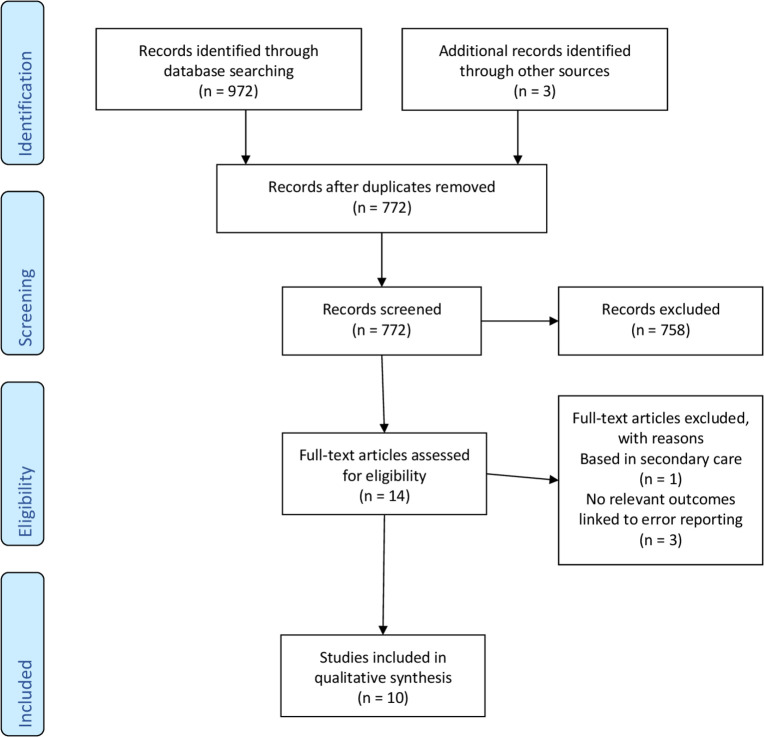
处方错误会对患者造成本可避免的伤害。大多数处方来自初级保健,在初级保健中,药物往往是自我施用的,错误最有可能造成伤害。报告处方错误可以识别趋势并减少事件再次发生的风险;然而,少报是很常见的。护理的组织和处方从一般做法到社区药房的运动可能会给专业人员有效地报告错误造成困难。这篇综述的目的是明确确定初级保健中处方错误报告的障碍和促进因素的初步研究。2019年7月完成了文献的系统研究。4个数据库(PubMed/Medline, Cochrane, CINAHL和Web of Science)检索相关研究。没有日期或语言限制。使用混合方法评估工具对符合条件的研究进行严格评估,并对数据进行描述性和叙述性综合。在最后的分析中包括了10篇文章。七项研究考虑了一般实践中的处方错误和错误报告,三项研究考虑了社区药房的设置。所纳入研究的结果分为五个主题,包括错误的定义、处方错误报告文化、报告程序、沟通和能力。医疗保健专业人员认识到处方错误报告的价值,但实施过程中存在主要障碍,包括时间、对报复的恐惧以及初级保健中的组织分离。
Prescribing error reporting in primary care: a narrative synthesis systematic review.
Prescribing errors can cause avoidable harm to patients. Most prescriptions originate in primary care, where medications tend to be self-administered and errors have the most potential to cause harm. Reporting prescribing errors can identify trends and reduce the risk of the reoccurrence of incidents; however, under-reporting is common. The organisation of care and the movement of prescriptions from general practice to community pharmacy may create difficulties for professionals to effectively report errors. This review aims specifically to identify primary research studies that examine barriers and facilitators to prescription error reporting across primary care. A systematic research of the literature was completed in July 2019. Four databases (PubMed/Medline, Cochrane, CINAHL and Web of Science) were searched for relevant studies. No date or language limits were applied. Eligible studies were critically appraised using the Mixed Methods Appraisal Tool, and data were descriptively and narratively synthesised. Ten articles were included in the final analysis. Seven studies considered prescription errors and error reporting within general practice and three within a community pharmacy setting. Findings from the included studies are presented across five themes, including definition of an error, prescribing error reporting culture, reporting processes, communication and capacity. Healthcare professionals appreciate the value of prescription error reporting, but there are key barriers to implementation, including time, fear of reprisal and organisation separation within primary care.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
