Patterns of Comorbidities and Prescribing and Dispensing of Non-steroidal Anti-inflammatory Drugs (NSAIDs) Among Patients with Osteoarthritis in the USA: Real-World Study.
Joshua Ide, Azza Shoaibi, Kerstin Wagner, Rachel Weinstein, Kathleen E Boyle, Andrew Myers
{"title":"Patterns of Comorbidities and Prescribing and Dispensing of Non-steroidal Anti-inflammatory Drugs (NSAIDs) Among Patients with Osteoarthritis in the USA: Real-World Study.","authors":"Joshua Ide, Azza Shoaibi, Kerstin Wagner, Rachel Weinstein, Kathleen E Boyle, Andrew Myers","doi":"10.1007/s40266-024-01108-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Osteoarthritis (OA) is a major cause of chronic pain. Non-steroidal anti-inflammatory drugs (NSAIDs) are analgesics commonly used for musculoskeletal pain; however, NSAIDs can increase the risk of certain adverse events, such as gastrointestinal bleeding, edema, heart failure, and hypertension.</p><p><strong>Objective: </strong>The objective of this study was to characterize existing comorbidities among patients with OA. For patients with OA with and without a coexisting medical condition of interest (CMCOI), we estimated the prevalence of prescribing and dispensing NSAIDs pre-OA and post-OA diagnosis.</p><p><strong>Methods: </strong>Data from three large administrative claims databases were used to construct an OA retrospective cohort. Databases leveraged were IBM MarketScan Medicare Supplemental Database (MDCR), IBM MarketScan Commercial Database (CCAE), and Optum's de-identified Clinformatics<sup>®</sup> Data Mart Database (Optum CDM). The OA study population was defined to be those patients who had an OA diagnosis from an inpatient or outpatient visit with at least 365 days of prior observation time in the database during January 2000 through May 2021. Asthma, cardiovascular disorders, renal impairment, and gastrointestinal bleeding risks were the CMCOI of interest. Patients with OA were then classified as having or not having evidence of a CMCOI. For both groups, NSAID dispensing patterns pre-OA and post-OA diagnosis were identified. Descriptive analysis was performed within the Observational Health Data Sciences and Informatics framework.</p><p><strong>Results: </strong>In each database, the proportion of the OA population with at least one CMCOI was nearly 50% or more (48.0% CCAE; 74.4% MDCR; 68.6% Optum CDM). Cardiovascular disease was the most commonly observed CMCOI in each database, and in two databases, nearly one in four patients with OA had two or more CMCOI (23.2% MDCR; 22.6% Optum CDM). Among the OA population with CMCOI, NSAID utilization post-OA diagnosis ranged from 33.0 to 46.2%. Following diagnosis of OA, an increase in the prescribing and dispensing of NSAIDs was observed in all databases, regardless of patient CMCOI presence.</p><p><strong>Conclusions: </strong>This study provides real-world evidence of the pattern of prescribing and dispensing of NSAIDs among patients with OA with and without CMCOI, which indicates that at least half of patients with OA in the USA have a coexisting condition. These conditions may increase the risk of side effects commonly associated with NSAIDs. Yet, at least 32% of these patients were prescribed and dispensed NSAIDs. These data support the importance of shared decision making between healthcare professionals and patients when considering NSAIDs for the treatment of OA in patients with NSAID-relevant coexisting medical conditions.</p>","PeriodicalId":11489,"journal":{"name":"Drugs & Aging","volume":" ","pages":"357-366"},"PeriodicalIF":3.8000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11021340/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Drugs & Aging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40266-024-01108-x","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/3/23 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Osteoarthritis (OA) is a major cause of chronic pain. Non-steroidal anti-inflammatory drugs (NSAIDs) are analgesics commonly used for musculoskeletal pain; however, NSAIDs can increase the risk of certain adverse events, such as gastrointestinal bleeding, edema, heart failure, and hypertension.
Objective: The objective of this study was to characterize existing comorbidities among patients with OA. For patients with OA with and without a coexisting medical condition of interest (CMCOI), we estimated the prevalence of prescribing and dispensing NSAIDs pre-OA and post-OA diagnosis.
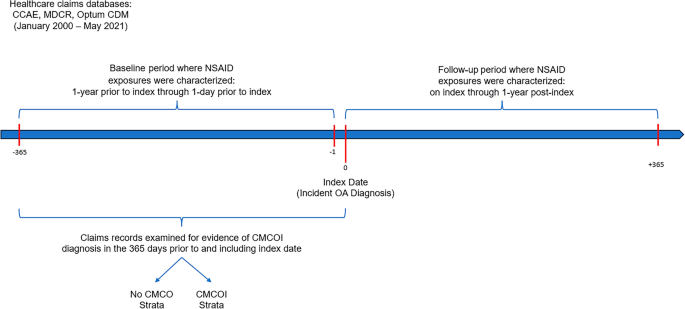
Methods: Data from three large administrative claims databases were used to construct an OA retrospective cohort. Databases leveraged were IBM MarketScan Medicare Supplemental Database (MDCR), IBM MarketScan Commercial Database (CCAE), and Optum's de-identified Clinformatics® Data Mart Database (Optum CDM). The OA study population was defined to be those patients who had an OA diagnosis from an inpatient or outpatient visit with at least 365 days of prior observation time in the database during January 2000 through May 2021. Asthma, cardiovascular disorders, renal impairment, and gastrointestinal bleeding risks were the CMCOI of interest. Patients with OA were then classified as having or not having evidence of a CMCOI. For both groups, NSAID dispensing patterns pre-OA and post-OA diagnosis were identified. Descriptive analysis was performed within the Observational Health Data Sciences and Informatics framework.
Results: In each database, the proportion of the OA population with at least one CMCOI was nearly 50% or more (48.0% CCAE; 74.4% MDCR; 68.6% Optum CDM). Cardiovascular disease was the most commonly observed CMCOI in each database, and in two databases, nearly one in four patients with OA had two or more CMCOI (23.2% MDCR; 22.6% Optum CDM). Among the OA population with CMCOI, NSAID utilization post-OA diagnosis ranged from 33.0 to 46.2%. Following diagnosis of OA, an increase in the prescribing and dispensing of NSAIDs was observed in all databases, regardless of patient CMCOI presence.
Conclusions: This study provides real-world evidence of the pattern of prescribing and dispensing of NSAIDs among patients with OA with and without CMCOI, which indicates that at least half of patients with OA in the USA have a coexisting condition. These conditions may increase the risk of side effects commonly associated with NSAIDs. Yet, at least 32% of these patients were prescribed and dispensed NSAIDs. These data support the importance of shared decision making between healthcare professionals and patients when considering NSAIDs for the treatment of OA in patients with NSAID-relevant coexisting medical conditions.
背景:骨关节炎(OA)是导致慢性疼痛的主要原因。非甾体类抗炎药(NSAIDs)是治疗肌肉骨骼疼痛的常用镇痛药;然而,非甾体类抗炎药会增加某些不良反应的风险,如胃肠道出血、水肿、心力衰竭和高血压:本研究旨在了解 OA 患者现有合并症的特征。对于有或没有并存相关疾病(CMCOI)的 OA 患者,我们估算了 OA 诊断前和诊断后开具和配发非甾体抗炎药的患病率:方法:我们利用三个大型行政索赔数据库的数据构建了一个 OA 回顾性队列。利用的数据库包括 IBM MarketScan 医疗保险补充数据库 (MDCR)、IBM MarketScan 商业数据库 (CCAE) 和 Optum 的去标识 Clinformatics® Data Mart 数据库 (Optum CDM)。OA 研究人群定义为 2000 年 1 月至 2021 年 5 月期间在数据库中至少观察了 365 天的住院或门诊患者中确诊为 OA 的患者。哮喘、心血管疾病、肾功能损害和胃肠道出血风险是研究关注的 CMCOI。然后将 OA 患者分为有 CMCOI 证据和无 CMCOI 证据两组。两组患者在确诊 OA 前和确诊 OA 后的非甾体抗炎药配药模式均已确定。在观察性健康数据科学和信息学框架内进行了描述性分析:在每个数据库中,至少患有一种CMCOI的OA人群比例接近50%或更高(CCAE为48.0%;MDCR为74.4%;Optum CDM为68.6%)。心血管疾病是每个数据库中最常见的 CMCOI,在两个数据库中,每四名 OA 患者中就有近一人患有两种或两种以上 CMCOI(23.2% MDCR;22.6% Optum CDM)。在有 CMCOI 的 OA 患者中,确诊 OA 后使用非甾体抗炎药的比例从 33.0% 到 46.2% 不等。诊断出 OA 后,无论患者是否存在 CMCOI,所有数据库中的非甾体抗炎药处方和配药量都有所增加:本研究提供了现实世界中存在和不存在 CMCOI 的 OA 患者的非甾体抗炎药处方和配药模式的证据,表明在美国至少有一半的 OA 患者同时患有其他疾病。这些疾病可能会增加非甾体抗炎药常见副作用的风险。然而,这些患者中至少有 32% 得到了非甾体抗炎药的处方和配药。这些数据支持医护人员和患者在考虑使用非甾体抗炎药治疗患有非甾体抗炎药相关并存病症的患者的 OA 时共同决策的重要性。
期刊介绍:
Drugs & Aging delivers essential information on the most important aspects of drug therapy to professionals involved in the care of the elderly.
The journal addresses in a timely way the major issues relating to drug therapy in older adults including: the management of specific diseases, particularly those associated with aging, age-related physiological changes impacting drug therapy, drug utilization and prescribing in the elderly, polypharmacy and drug interactions.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
