{"title":"Double novel integrated outside biliary stent and nasobiliary drainage catheter system placement for hilar biliary stricture","authors":"Akihiro Sekine, Kazunari Nakahara, Keisuke Tateishi","doi":"10.1111/den.14799","DOIUrl":null,"url":null,"abstract":"<p>A novel integrated biliary stent and nasobiliary drainage catheter system (UMIDAS NB stent [UMIDAS]; Olympus Medical Systems, Tokyo, Japan) was recently renewed.<span><sup>1, 2</sup></span> The renewed UMIDAS consists of a 7F or 8.5F outside biliary stent with a large flap on the distal side to prevent migration and a 5F nasobiliary catheter (Fig. 1). The advantage of the UMIDAS is that additional endoscopic retrograde cholangiopancreatography is not required because internal drainage can be achieved by simply removing the nasobiliary catheter.<span><sup>3, 4</sup></span> However, because of the large 8.5F diameter of the stent pushing sheath, it is impossible to deploy two UMIDASs through the scope channel. Here, we present a technique demonstrating the placement of two UMIDASs (Video S1).</p><p>External drainage of the right anterior and posterior bile ducts was planned before left hepatic lobectomy for hilar biliary stricture resulting from cholangiocarcinoma. Endoscopic retrograde cholangiopancreatography was performed using a duodenoscope (TJF-Q290V; Olympus Medical Systems). After bile duct cannulation, 0.025 inch guidewires were inserted into the anterior and posterior branches, followed by endoscopic sphincterotomy. Next, a UMIDAS with a 7F biliary stent was inserted into the anterior branch across the papilla. Because a second UMIDAS could not be inserted through the 4.2 mm diameter scope channel, pushing sheath and nasocatheter of the first UMIDAS were temporarily removed while retaining the biliary stent and guidewire in place (Fig. 2a). This allowed the second UMIDAS to be inserted through the channel and placed in the posterior branch (Fig. 2b). After removing the pushing sheath of the second UMIDAS, the nasocatheter of the first UMIDAS was reinserted through the lumen of the biliary stent and placed in the anterior branch (Fig. 2c,d).</p><p>A week later, the nasobiliary catheters were successfully extracted under fluoroscopic guidance while the biliary stents were retained in place.</p><p>Authors declare no conflict of interest for this article.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 6","pages":"740-741"},"PeriodicalIF":4.7000,"publicationDate":"2024-04-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14799","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14799","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
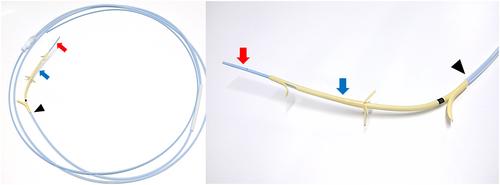
A novel integrated biliary stent and nasobiliary drainage catheter system (UMIDAS NB stent [UMIDAS]; Olympus Medical Systems, Tokyo, Japan) was recently renewed.1, 2 The renewed UMIDAS consists of a 7F or 8.5F outside biliary stent with a large flap on the distal side to prevent migration and a 5F nasobiliary catheter (Fig. 1). The advantage of the UMIDAS is that additional endoscopic retrograde cholangiopancreatography is not required because internal drainage can be achieved by simply removing the nasobiliary catheter.3, 4 However, because of the large 8.5F diameter of the stent pushing sheath, it is impossible to deploy two UMIDASs through the scope channel. Here, we present a technique demonstrating the placement of two UMIDASs (Video S1).
External drainage of the right anterior and posterior bile ducts was planned before left hepatic lobectomy for hilar biliary stricture resulting from cholangiocarcinoma. Endoscopic retrograde cholangiopancreatography was performed using a duodenoscope (TJF-Q290V; Olympus Medical Systems). After bile duct cannulation, 0.025 inch guidewires were inserted into the anterior and posterior branches, followed by endoscopic sphincterotomy. Next, a UMIDAS with a 7F biliary stent was inserted into the anterior branch across the papilla. Because a second UMIDAS could not be inserted through the 4.2 mm diameter scope channel, pushing sheath and nasocatheter of the first UMIDAS were temporarily removed while retaining the biliary stent and guidewire in place (Fig. 2a). This allowed the second UMIDAS to be inserted through the channel and placed in the posterior branch (Fig. 2b). After removing the pushing sheath of the second UMIDAS, the nasocatheter of the first UMIDAS was reinserted through the lumen of the biliary stent and placed in the anterior branch (Fig. 2c,d).
A week later, the nasobiliary catheters were successfully extracted under fluoroscopic guidance while the biliary stents were retained in place.
Authors declare no conflict of interest for this article.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
