Sukhvir Kaur, Kathleen Boström, Anneke Ullrich, Nikolas Oubaid, Karin Oechsle, Holger Schulz, Raymond Voltz, Kerstin Kremeike
{"title":"Health Experts’ Perspectives on Barriers, Facilitators, and Needs for Improvement of Hospital Care in the Dying Phase","authors":"Sukhvir Kaur, Kathleen Boström, Anneke Ullrich, Nikolas Oubaid, Karin Oechsle, Holger Schulz, Raymond Voltz, Kerstin Kremeike","doi":"10.1155/2024/1012971","DOIUrl":null,"url":null,"abstract":"<div>\n <p><i>Introduction</i>. Globally, hospitals are an important place in end-of-life care and most frequent place of death in Germany (47%), but at the same time, the least preferred one—both for patients and their informal caregivers. As hospital care in the dying phase on non-palliative care wards has rarely been studied systematically, we assessed the current state of care in the dying phase in hospitals as a first step. <i>Methods</i>. In an online survey, <i>N</i> = 165 national health experts were invited to answer eight open questions on care aspects, facilitators, barriers, and needs for improvement as well as COVID-19 pandemic specifics regarding hospital care in the dying phase. Sociodemographic data were analysed descriptively, and responses were analysed using qualitative thematic analysis. <i>Results</i>. Of <i>n</i> = 65 experts, 52% work as nursing staff and 30% as physicians. We identified facilitators, barriers, and needs for improvement regarding 11 topics on the following three levels: institutional level (general institutional conditions, hospital culture, and integration of specialist palliative care), team level (attitude towards and dealing with death and dying, competencies, communication, and teamwork) and care level (dying phase, symptom control, patient centredness, and involvement of informal caregivers). <i>Conclusion</i>. Improving care in the dying phase has to overcome barriers on various levels. We assume that rather “small” measures will find their way into clinical routine and contribute to the improvement of hospital care in the dying phase.</p>\n </div>","PeriodicalId":13782,"journal":{"name":"International Journal of Clinical Practice","volume":"2024 1","pages":""},"PeriodicalIF":2.4000,"publicationDate":"2024-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/1012971","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Clinical Practice","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1155/2024/1012971","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
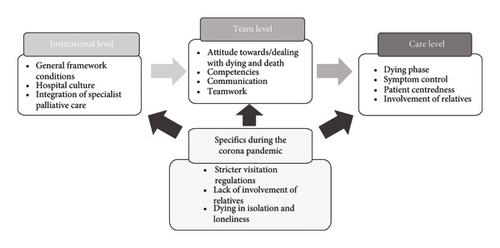
Introduction. Globally, hospitals are an important place in end-of-life care and most frequent place of death in Germany (47%), but at the same time, the least preferred one—both for patients and their informal caregivers. As hospital care in the dying phase on non-palliative care wards has rarely been studied systematically, we assessed the current state of care in the dying phase in hospitals as a first step. Methods. In an online survey, N = 165 national health experts were invited to answer eight open questions on care aspects, facilitators, barriers, and needs for improvement as well as COVID-19 pandemic specifics regarding hospital care in the dying phase. Sociodemographic data were analysed descriptively, and responses were analysed using qualitative thematic analysis. Results. Of n = 65 experts, 52% work as nursing staff and 30% as physicians. We identified facilitators, barriers, and needs for improvement regarding 11 topics on the following three levels: institutional level (general institutional conditions, hospital culture, and integration of specialist palliative care), team level (attitude towards and dealing with death and dying, competencies, communication, and teamwork) and care level (dying phase, symptom control, patient centredness, and involvement of informal caregivers). Conclusion. Improving care in the dying phase has to overcome barriers on various levels. We assume that rather “small” measures will find their way into clinical routine and contribute to the improvement of hospital care in the dying phase.
期刊介绍:
IJCP is a general medical journal. IJCP gives special priority to work that has international appeal.
IJCP publishes:
Editorials. IJCP Editorials are commissioned. [Peer reviewed at the editor''s discretion]
Perspectives. Most IJCP Perspectives are commissioned. Example. [Peer reviewed at the editor''s discretion]
Study design and interpretation. Example. [Always peer reviewed]
Original data from clinical investigations. In particular: Primary research papers from RCTs, observational studies, epidemiological studies; pre-specified sub-analyses; pooled analyses. [Always peer reviewed]
Meta-analyses. [Always peer reviewed]
Systematic reviews. From October 2009, special priority will be given to systematic reviews. [Always peer reviewed]
Non-systematic/narrative reviews. From October 2009, reviews that are not systematic will be considered only if they include a discrete Methods section that must explicitly describe the authors'' approach. Special priority will, however, be given to systematic reviews. [Always peer reviewed]
''How to…'' papers. Example. [Always peer reviewed]
Consensus statements. [Always peer reviewed] Short reports. [Always peer reviewed]
Letters. [Peer reviewed at the editor''s discretion]
International scope
IJCP publishes work from investigators globally. Around 30% of IJCP articles list an author from the UK. Around 30% of IJCP articles list an author from the USA or Canada. Around 45% of IJCP articles list an author from a European country that is not the UK. Around 15% of articles published in IJCP list an author from a country in the Asia-Pacific region.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
