Anjun Chen, Erman Wu, Ran Huang, Bairong Shen, Ruobing Han, Jian Wen, Zhiyong Zhang, Qinghua Li
{"title":"Development of Lung Cancer Risk Prediction Machine Learning Models for Equitable Learning Health System: Retrospective Study.","authors":"Anjun Chen, Erman Wu, Ran Huang, Bairong Shen, Ruobing Han, Jian Wen, Zhiyong Zhang, Qinghua Li","doi":"10.2196/56590","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A significant proportion of young at-risk patients and nonsmokers are excluded by the current guidelines for lung cancer (LC) screening, resulting in low-screening adoption. The vision of the US National Academy of Medicine to transform health systems into learning health systems (LHS) holds promise for bringing necessary structural changes to health care, thereby addressing the exclusivity and adoption issues of LC screening.</p><p><strong>Objective: </strong>This study aims to realize the LHS vision by designing an equitable, machine learning (ML)-enabled LHS unit for LC screening. It focuses on developing an inclusive and practical LC risk prediction model, suitable for initializing the ML-enabled LHS (ML-LHS) unit. This model aims to empower primary physicians in a clinical research network, linking central hospitals and rural clinics, to routinely deliver risk-based screening for enhancing LC early detection in broader populations.</p><p><strong>Methods: </strong>We created a standardized data set of health factors from 1397 patients with LC and 1448 control patients, all aged 30 years and older, including both smokers and nonsmokers, from a hospital's electronic medical record system. Initially, a data-centric ML approach was used to create inclusive ML models for risk prediction from all available health factors. Subsequently, a quantitative distribution of LC health factors was used in feature engineering to refine the models into a more practical model with fewer variables.</p><p><strong>Results: </strong>The initial inclusive 250-variable XGBoost model for LC risk prediction achieved performance metrics of 0.86 recall, 0.90 precision, and 0.89 accuracy. Post feature refinement, a practical 29-variable XGBoost model was developed, displaying performance metrics of 0.80 recall, 0.82 precision, and 0.82 accuracy. This model met the criteria for initializing the ML-LHS unit for risk-based, inclusive LC screening within clinical research networks.</p><p><strong>Conclusions: </strong>This study designed an innovative ML-LHS unit for a clinical research network, aiming to sustainably provide inclusive LC screening to all at-risk populations. It developed an inclusive and practical XGBoost model from hospital electronic medical record data, capable of initializing such an ML-LHS unit for community and rural clinics. The anticipated deployment of this ML-LHS unit is expected to significantly improve LC-screening rates and early detection among broader populations, including those typically overlooked by existing screening guidelines.</p>","PeriodicalId":73551,"journal":{"name":"JMIR AI","volume":"3 ","pages":"e56590"},"PeriodicalIF":2.0000,"publicationDate":"2024-09-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11425024/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR AI","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/56590","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A significant proportion of young at-risk patients and nonsmokers are excluded by the current guidelines for lung cancer (LC) screening, resulting in low-screening adoption. The vision of the US National Academy of Medicine to transform health systems into learning health systems (LHS) holds promise for bringing necessary structural changes to health care, thereby addressing the exclusivity and adoption issues of LC screening.
Objective: This study aims to realize the LHS vision by designing an equitable, machine learning (ML)-enabled LHS unit for LC screening. It focuses on developing an inclusive and practical LC risk prediction model, suitable for initializing the ML-enabled LHS (ML-LHS) unit. This model aims to empower primary physicians in a clinical research network, linking central hospitals and rural clinics, to routinely deliver risk-based screening for enhancing LC early detection in broader populations.
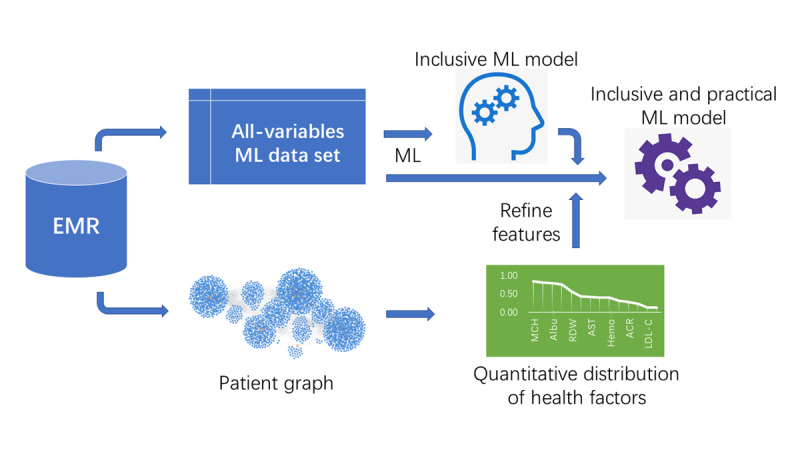
Methods: We created a standardized data set of health factors from 1397 patients with LC and 1448 control patients, all aged 30 years and older, including both smokers and nonsmokers, from a hospital's electronic medical record system. Initially, a data-centric ML approach was used to create inclusive ML models for risk prediction from all available health factors. Subsequently, a quantitative distribution of LC health factors was used in feature engineering to refine the models into a more practical model with fewer variables.
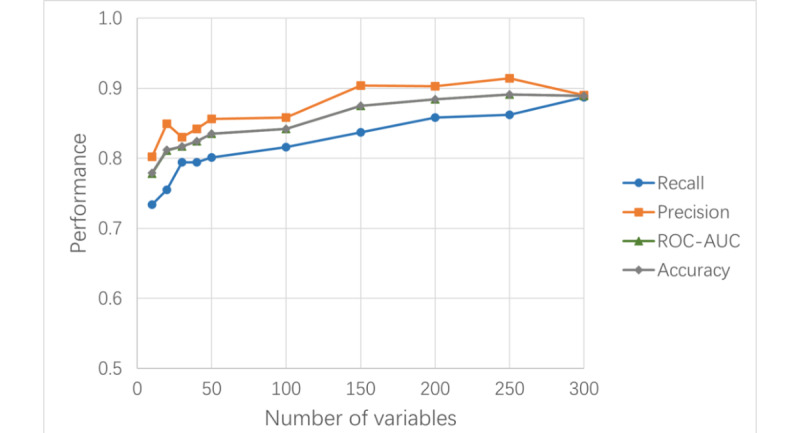
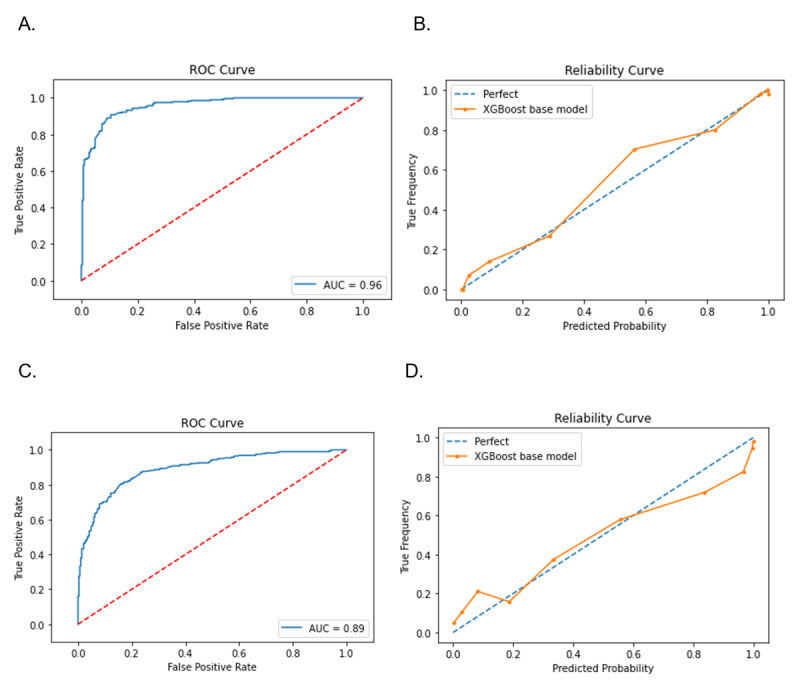
Results: The initial inclusive 250-variable XGBoost model for LC risk prediction achieved performance metrics of 0.86 recall, 0.90 precision, and 0.89 accuracy. Post feature refinement, a practical 29-variable XGBoost model was developed, displaying performance metrics of 0.80 recall, 0.82 precision, and 0.82 accuracy. This model met the criteria for initializing the ML-LHS unit for risk-based, inclusive LC screening within clinical research networks.
Conclusions: This study designed an innovative ML-LHS unit for a clinical research network, aiming to sustainably provide inclusive LC screening to all at-risk populations. It developed an inclusive and practical XGBoost model from hospital electronic medical record data, capable of initializing such an ML-LHS unit for community and rural clinics. The anticipated deployment of this ML-LHS unit is expected to significantly improve LC-screening rates and early detection among broader populations, including those typically overlooked by existing screening guidelines.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
