{"title":"Ruxolitinib plus steroids for acute graft versus host disease: a multicenter, randomized, phase 3 trial","authors":"Liping Dou, Yanli Zhao, Jingjing Yang, Lei Deng, Nan Wang, Xiawei Zhang, Qingyang Liu, Yan Yang, Zhijie Wei, Fuxu Wang, Yifan Jiao, Fei Li, Songhua Luan, Liangding Hu, Sujun Gao, Chuanfang Liu, Xiangjun Liu, Jinsong Yan, Xuejun Zhang, Fang Zhou, Peihua Lu, Daihong Liu","doi":"10.1038/s41392-024-01987-x","DOIUrl":null,"url":null,"abstract":"<p>Newly diagnosed patients with high-risk acute graft-versus-host disease (aGVHD) often experience poor clinical outcomes and low complete remission rates. Ruxolitinib with corticosteroids showed promising efficacy in improving response and failure free survival in our phase I study. This study (ClinicalTrials.gov: NCT04061876) sought to evaluate the safety and effectiveness of combining ruxolitinib (RUX, 5 mg/day) with corticosteroids (1 mg/kg/day methylprednisolone, RUX/steroids combined group) versus using methylprednisolone alone (2 mg/kg/day, steroids-only group). Newly diagnosed patients with intermediate- or high-risk aGVHD were included, with risk levels classified by either the Minnesota aGVHD Risk Score or biomarker assessment. Patients were randomized in a ratio of 1:1 into 2 groups: 99 patients received RUX combined with methylprednisolone, while the other 99 received methylprednisolone alone as the initial treatment. The RUX/steroids group showed a significantly higher overall response rate (ORR) on day 28 (92.9%) compared to the steroids-only group (70.7%, Odds Ratio [OR] = 5.8; 95% Confidence Interval [CI], 2.4–14.0; <i>P</i> < 0.001). Similarly, the ORR on day 56 was higher in the RUX/steroids group (85.9% vs. 46.5%; OR = 7.07; 95% CI, 3.36–15.75; <i>P</i> < 0.001). Additionally, the 18-month failure-free survival was significantly better in the RUX/steroids group (57.2%) compared to the steroids-only group (33.3%; Hazard Ratio = 0.46; 95% CI, 0.31–0.68; <i>P</i> < 0.001). Adverse events (AEs) frequencies were comparable between both groups, with the exception of fewer grade 4 AEs in the RUX/steroids group (26.3% vs. 50.5% <i>P</i> = 0.005). To our knowledge, this study is the first prospective, randomized controlled trial to demonstrate that adding ruxolitinib to the standard methylprednisolone regimen provides an effective and safe first-line treatment for newly diagnosed high-risk acute GVHD.</p>","PeriodicalId":21766,"journal":{"name":"Signal Transduction and Targeted Therapy","volume":"1 1","pages":""},"PeriodicalIF":52.7000,"publicationDate":"2024-10-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Signal Transduction and Targeted Therapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41392-024-01987-x","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
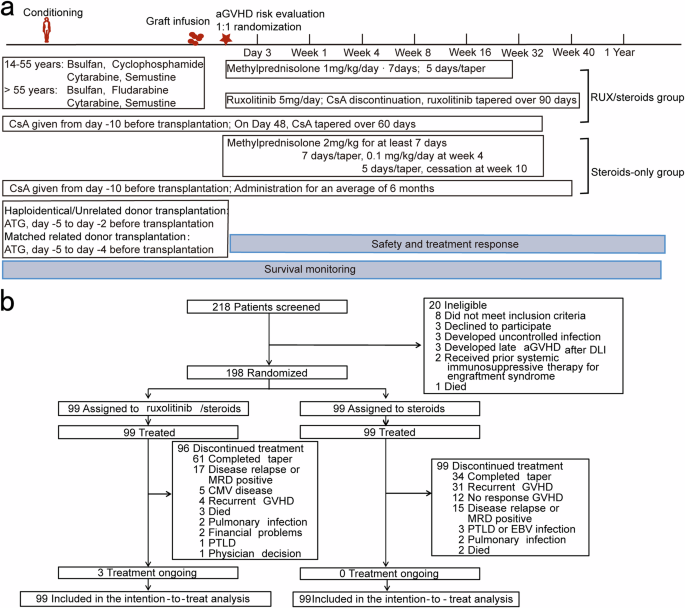
Newly diagnosed patients with high-risk acute graft-versus-host disease (aGVHD) often experience poor clinical outcomes and low complete remission rates. Ruxolitinib with corticosteroids showed promising efficacy in improving response and failure free survival in our phase I study. This study (ClinicalTrials.gov: NCT04061876) sought to evaluate the safety and effectiveness of combining ruxolitinib (RUX, 5 mg/day) with corticosteroids (1 mg/kg/day methylprednisolone, RUX/steroids combined group) versus using methylprednisolone alone (2 mg/kg/day, steroids-only group). Newly diagnosed patients with intermediate- or high-risk aGVHD were included, with risk levels classified by either the Minnesota aGVHD Risk Score or biomarker assessment. Patients were randomized in a ratio of 1:1 into 2 groups: 99 patients received RUX combined with methylprednisolone, while the other 99 received methylprednisolone alone as the initial treatment. The RUX/steroids group showed a significantly higher overall response rate (ORR) on day 28 (92.9%) compared to the steroids-only group (70.7%, Odds Ratio [OR] = 5.8; 95% Confidence Interval [CI], 2.4–14.0; P < 0.001). Similarly, the ORR on day 56 was higher in the RUX/steroids group (85.9% vs. 46.5%; OR = 7.07; 95% CI, 3.36–15.75; P < 0.001). Additionally, the 18-month failure-free survival was significantly better in the RUX/steroids group (57.2%) compared to the steroids-only group (33.3%; Hazard Ratio = 0.46; 95% CI, 0.31–0.68; P < 0.001). Adverse events (AEs) frequencies were comparable between both groups, with the exception of fewer grade 4 AEs in the RUX/steroids group (26.3% vs. 50.5% P = 0.005). To our knowledge, this study is the first prospective, randomized controlled trial to demonstrate that adding ruxolitinib to the standard methylprednisolone regimen provides an effective and safe first-line treatment for newly diagnosed high-risk acute GVHD.
新确诊的高危急性移植物抗宿主病(aGVHD)患者往往临床疗效不佳,完全缓解率低。在我们的 I 期研究中,Ruxolitinib 联合皮质类固醇治疗在改善反应和无失败生存期方面显示出良好的疗效。这项研究(ClinicalTrials.gov:NCT04061876)旨在评估Ruxolitinib(RUX,5毫克/天)与皮质类固醇(1毫克/公斤/天甲基强的松龙,RUX/皮质类固醇联合组)联合治疗与单独使用甲基强的松龙(2毫克/公斤/天,仅使用皮质类固醇组)的安全性和有效性。新确诊的中危或高危 aGVHD 患者均被纳入其中,风险等级根据明尼苏达 aGVHD 风险评分或生物标志物评估进行分类。患者按1:1的比例随机分为两组:99名患者接受RUX联合甲基强的松龙治疗,另外99名患者则接受单纯甲基强的松龙作为初始治疗。RUX/类固醇组第28天的总反应率(ORR)(92.9%)明显高于单纯类固醇组(70.7%,Odds Ratio [OR] = 5.8; 95% Confidence Interval [CI], 2.4-14.0; P < 0.001)。同样,RUX/类固醇组第56天的ORR也更高(85.9% vs. 46.5%;OR = 7.07;95% CI, 3.36-15.75; P <0.001)。此外,与单纯类固醇组(33.3%;危险比=0.46;95% CI,0.31-0.68;P <0.001)相比,RUX/类固醇组的18个月无失败生存率(57.2%)明显更高。两组的不良事件(AEs)发生率相当,但RUX/类固醇组的4级不良事件较少(26.3% vs. 50.5% P = 0.005)。据我们所知,该研究是首个前瞻性随机对照试验,证明在标准甲泼尼龙方案中加入鲁索利替尼可为新诊断的高危急性GVHD患者提供有效、安全的一线治疗。
期刊介绍:
Signal Transduction and Targeted Therapy is an open access journal that focuses on timely publication of cutting-edge discoveries and advancements in basic science and clinical research related to signal transduction and targeted therapy.
Scope: The journal covers research on major human diseases, including, but not limited to:
Cancer,Cardiovascular diseases,Autoimmune diseases,Nervous system diseases.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
