Courtney W Chan, Leo K Westgard, Andrew Romasco, Krisztian Gado, Shira Doron, Maya L Nadimpalli
{"title":"Sociodemographic disparities in antibiotic-resistant outpatient urine cultures in a Boston hospital, 2015-2020: a cross-sectional analysis.","authors":"Courtney W Chan, Leo K Westgard, Andrew Romasco, Krisztian Gado, Shira Doron, Maya L Nadimpalli","doi":"10.1186/s12939-024-02308-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Antibiotic resistance in uropathogens has rapidly escalated over time, complicating treatment and increasing morbidity and mortality. Few studies have explored how the social determinants of health may be associated with patients' risks for acquiring antibiotic-resistant (AR) uropathogens.</p><p><strong>Methods: </strong>We identified urine cultures collected from outpatients presenting to Tufts Medical Center Primary Care Practices between 2015 and 2020. Specimens were included if patients' age, sex, and residential address were recorded in the electronic medical record (EMR) and if their urine culture yielded Enterococcus spp. or one or more gram-negative bacterial organism(s) or for which antibiotic susceptibility profiling and species identification was conducted. We abstracted patients' sociodemographic characteristics from the EMR and used US Census Bureau data to identify characteristics about patients' census tracts of residence. We evaluated associations between individual- and neighborhood-level characteristics and patients' risk of having a urine culture resistant to (1) three or more antibiotic classes (i.e., multidrug resistant [MDR]), (2) first-line treatments, (3) fluoroquinolones, (4) aminoglycosides, or (5) ceftriaxone using logistic regression models and a Bonferroni correction to account for multiple hypothesis testing.</p><p><strong>Results: </strong>We included urine cultures from 1,306 unique outpatients, most of whom were female (89%). Patients largely self-identified as Non-Hispanic White (36%), Asian (15%), or Non-Hispanic Black (11%). Over 60% lived in an environmental justice-designated census tract. Most included isolates were Escherichia coli (76%) or Klebsiella pneumoniae (7%). Using public insurance increased patients' odds of having a uropathogen resistant to first-line antibiotics, but living in a limited-income neighborhood reduced patients' odds of having a MDR uropathogen by 47%. We noted a strong but non-significant positive trend between speaking a language other than English and having an aminoglycoside-resistant uropathogen (p-value = 0.02). Most notably, after controlling for other factors, we observed no statistically significant associations between race or ethnicity and AR uropathogens.</p><p><strong>Conclusion: </strong>The social determinants of health may play important and intersecting roles in determining a patient's risk of having a resistant uropathogens that is more challenging or expensive to treat. It is crucial to acknowledge how race is likely to be a proxy for other factors affecting health, and to consider that some groups may be disproportionately impacted by antibiotic resistance.</p>","PeriodicalId":13745,"journal":{"name":"International Journal for Equity in Health","volume":"23 1","pages":"219"},"PeriodicalIF":4.1000,"publicationDate":"2024-10-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11520160/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal for Equity in Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12939-024-02308-y","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Antibiotic resistance in uropathogens has rapidly escalated over time, complicating treatment and increasing morbidity and mortality. Few studies have explored how the social determinants of health may be associated with patients' risks for acquiring antibiotic-resistant (AR) uropathogens.
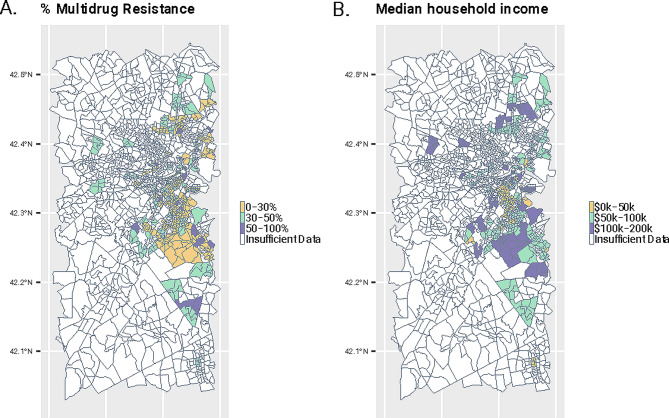
Methods: We identified urine cultures collected from outpatients presenting to Tufts Medical Center Primary Care Practices between 2015 and 2020. Specimens were included if patients' age, sex, and residential address were recorded in the electronic medical record (EMR) and if their urine culture yielded Enterococcus spp. or one or more gram-negative bacterial organism(s) or for which antibiotic susceptibility profiling and species identification was conducted. We abstracted patients' sociodemographic characteristics from the EMR and used US Census Bureau data to identify characteristics about patients' census tracts of residence. We evaluated associations between individual- and neighborhood-level characteristics and patients' risk of having a urine culture resistant to (1) three or more antibiotic classes (i.e., multidrug resistant [MDR]), (2) first-line treatments, (3) fluoroquinolones, (4) aminoglycosides, or (5) ceftriaxone using logistic regression models and a Bonferroni correction to account for multiple hypothesis testing.
Results: We included urine cultures from 1,306 unique outpatients, most of whom were female (89%). Patients largely self-identified as Non-Hispanic White (36%), Asian (15%), or Non-Hispanic Black (11%). Over 60% lived in an environmental justice-designated census tract. Most included isolates were Escherichia coli (76%) or Klebsiella pneumoniae (7%). Using public insurance increased patients' odds of having a uropathogen resistant to first-line antibiotics, but living in a limited-income neighborhood reduced patients' odds of having a MDR uropathogen by 47%. We noted a strong but non-significant positive trend between speaking a language other than English and having an aminoglycoside-resistant uropathogen (p-value = 0.02). Most notably, after controlling for other factors, we observed no statistically significant associations between race or ethnicity and AR uropathogens.
Conclusion: The social determinants of health may play important and intersecting roles in determining a patient's risk of having a resistant uropathogens that is more challenging or expensive to treat. It is crucial to acknowledge how race is likely to be a proxy for other factors affecting health, and to consider that some groups may be disproportionately impacted by antibiotic resistance.
期刊介绍:
International Journal for Equity in Health is an Open Access, peer-reviewed, online journal presenting evidence relevant to the search for, and attainment of, equity in health across and within countries. International Journal for Equity in Health aims to improve the understanding of issues that influence the health of populations. This includes the discussion of political, policy-related, economic, social and health services-related influences, particularly with regard to systematic differences in distributions of one or more aspects of health in population groups defined demographically, geographically, or socially.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
