{"title":"Hemodynamic Alterations in Cardiac Function Among Patients With Stroke and SARS-CoV-2 Infection: A Retrospective Cohort Study","authors":"Mingchao Zhou, Fubing Zha, Liuyang Zhao, Dongxia Li, Jiao Luo, Yao Wang, Fang Liu, Jing Zhou, Zeyu Zhang, Yucong Zou, Feng Xiong, Dianrui Hou, Fei Li, Mingjun He, Yongjie Zhu, Yulong Wang","doi":"10.1155/2024/2047103","DOIUrl":null,"url":null,"abstract":"<div>\n <p><b>Objective:</b> Cardiovascular complications associated with COVID-19 are being increasingly recognized. They include potential long-term effects on the heart, although how these complications manifest in patients with stroke who are already vulnerable to cardiovascular issues is lacking. This study addressed this gap by investigating the influence of SARS-CoV-2 infection on cardiac hemodynamic changes in inpatients with stroke, thereby providing valuable insights into the management of cardiac complications in this population.</p>\n <p><b>Methods:</b> This retrospective cohort study enrolled inpatients with stroke who did or did not experience SARS-CoV-2 infection in Shenzhen Second People’s Hospital. Clinical information, hemodynamics data, serum myocardial enzyme levels, functional levels, including Barthel index, and Longshi scale assessment (bedridden, domestic, and community) were extracted from clinical records. An independent sample <i>t</i>-test and the Mann–Whitney <i>U</i> test were used for comparison between groups. Multiple logistic regression analysis was used to identify indicators associated with decline in cardiac function in patients with stroke post-COVID-19.</p>\n <p><b>Results:</b> Eighty-three patients with stroke (average age of 66.0 ± 15.5 years) were recruited (42 patients in the study group and 41 in the control group). No significant difference in general characteristics was observed between the groups. The ejection fraction (EF, 56.45 ± 12.46 vs. 47.64 ± 14.76, <i>p</i> = 0.04) was decreased, and the end-diastolic volume (EDV, 142.74 ± 80.00 vs. 193.34 ± 140.17, <i>p</i> = 0.001) was increased significantly in patients infected with SARS-CoV-2 compared with the noninfected participants. SARS-CoV-2 infection was an independent risk factor for EF (−10%) decrease (OR: 5.205, 95% CI: 1.621–16.720, <i>p</i> = 0.006). The risk of cardiac function decline among bedridden infected patients was 15.43 times higher than that of uninfected nonbedridden patients (OR: 15.430, 95% CI: 1.402–169.805, <i>p</i> = 0.025).</p>\n <p><b>Conclusion:</b> Patients who are bedridden after stroke face a higher potential risk of cardiac hemodynamic impairment following SARS-CoV-2 infection, emphasizing the need for meticulous hemodynamic monitoring during treatment and rehabilitation of these patients to prevent any potential cardiovascular complications.</p>\n <p><b>Trial Registration:</b> ClinicalTrials.gov identifier: ChiCTR2300071376.</p>\n </div>","PeriodicalId":13782,"journal":{"name":"International Journal of Clinical Practice","volume":"2024 1","pages":""},"PeriodicalIF":2.4000,"publicationDate":"2024-11-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1155/2024/2047103","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Clinical Practice","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1155/2024/2047103","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Cardiovascular complications associated with COVID-19 are being increasingly recognized. They include potential long-term effects on the heart, although how these complications manifest in patients with stroke who are already vulnerable to cardiovascular issues is lacking. This study addressed this gap by investigating the influence of SARS-CoV-2 infection on cardiac hemodynamic changes in inpatients with stroke, thereby providing valuable insights into the management of cardiac complications in this population.
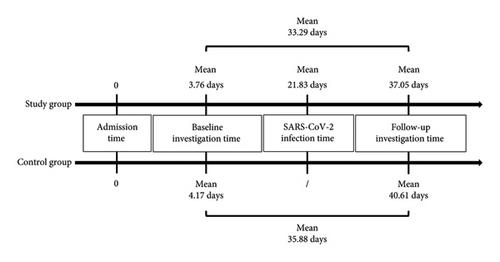
Methods: This retrospective cohort study enrolled inpatients with stroke who did or did not experience SARS-CoV-2 infection in Shenzhen Second People’s Hospital. Clinical information, hemodynamics data, serum myocardial enzyme levels, functional levels, including Barthel index, and Longshi scale assessment (bedridden, domestic, and community) were extracted from clinical records. An independent sample t-test and the Mann–Whitney U test were used for comparison between groups. Multiple logistic regression analysis was used to identify indicators associated with decline in cardiac function in patients with stroke post-COVID-19.
Results: Eighty-three patients with stroke (average age of 66.0 ± 15.5 years) were recruited (42 patients in the study group and 41 in the control group). No significant difference in general characteristics was observed between the groups. The ejection fraction (EF, 56.45 ± 12.46 vs. 47.64 ± 14.76, p = 0.04) was decreased, and the end-diastolic volume (EDV, 142.74 ± 80.00 vs. 193.34 ± 140.17, p = 0.001) was increased significantly in patients infected with SARS-CoV-2 compared with the noninfected participants. SARS-CoV-2 infection was an independent risk factor for EF (−10%) decrease (OR: 5.205, 95% CI: 1.621–16.720, p = 0.006). The risk of cardiac function decline among bedridden infected patients was 15.43 times higher than that of uninfected nonbedridden patients (OR: 15.430, 95% CI: 1.402–169.805, p = 0.025).
Conclusion: Patients who are bedridden after stroke face a higher potential risk of cardiac hemodynamic impairment following SARS-CoV-2 infection, emphasizing the need for meticulous hemodynamic monitoring during treatment and rehabilitation of these patients to prevent any potential cardiovascular complications.
期刊介绍:
IJCP is a general medical journal. IJCP gives special priority to work that has international appeal.
IJCP publishes:
Editorials. IJCP Editorials are commissioned. [Peer reviewed at the editor''s discretion]
Perspectives. Most IJCP Perspectives are commissioned. Example. [Peer reviewed at the editor''s discretion]
Study design and interpretation. Example. [Always peer reviewed]
Original data from clinical investigations. In particular: Primary research papers from RCTs, observational studies, epidemiological studies; pre-specified sub-analyses; pooled analyses. [Always peer reviewed]
Meta-analyses. [Always peer reviewed]
Systematic reviews. From October 2009, special priority will be given to systematic reviews. [Always peer reviewed]
Non-systematic/narrative reviews. From October 2009, reviews that are not systematic will be considered only if they include a discrete Methods section that must explicitly describe the authors'' approach. Special priority will, however, be given to systematic reviews. [Always peer reviewed]
''How to…'' papers. Example. [Always peer reviewed]
Consensus statements. [Always peer reviewed] Short reports. [Always peer reviewed]
Letters. [Peer reviewed at the editor''s discretion]
International scope
IJCP publishes work from investigators globally. Around 30% of IJCP articles list an author from the UK. Around 30% of IJCP articles list an author from the USA or Canada. Around 45% of IJCP articles list an author from a European country that is not the UK. Around 15% of articles published in IJCP list an author from a country in the Asia-Pacific region.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
