Contribution of point-of-care ultrasound in the prehospital management of patients with non-trauma acute dyspnea: a systematic review and meta-analysis.
{"title":"Contribution of point-of-care ultrasound in the prehospital management of patients with non-trauma acute dyspnea: a systematic review and meta-analysis.","authors":"Omide Taheri, Julie Samain, Frédéric Mauny, Marc Puyraveau, Thibaut Desmettre, Tania Marx","doi":"10.1097/MEJ.0000000000001205","DOIUrl":null,"url":null,"abstract":"<p><p>Acute dyspnea is a common symptom whose management is challenging in prehospital settings. Point-of-care ultrasound (POCUS) is increasingly accessible because of device miniaturization. To assess the contribution of POCUS in the prehospital management of patients with acute nontraumatic dyspnea, we performed a systematic review on nontrauma patients of any age managed in the prehospital setting for acute dyspnea and receiving a POCUS examination. We searched seven databases and gray literature for English-language studies published from January 1995 to November 2023. Two independent reviewers completed the study selection, data extraction, and risk of bias assessment. The primary outcome was the assessment of the contribution of POCUS to feasibility, diagnostic, therapeutic, prognosis, patient referral, and transport vector modification. Twenty-three studies were included. The risk of bias assessment identified 3 intermediate-risk, 18 serious-risk, and 2 critical-risk studies. Three studies reported moderate to excellent feasibility for lung POCUS, and three studies reported poor to mediocre feasibility for cardiac POCUS. The median duration of the POCUS examination was less than 5 minutes (six studies). POCUS improved diagnostic identification (seven studies). The diagnostic accuracy of POCUS was excellent for pneumothorax (sensitivity = 100%, specificity = 100%, two studies), very good for acute heart failure (sensitivity = 71-100%, specificity = 72-95%, eight studies), good for pneumonia (sensitivity = 88%, specificity = 59%, one study), and moderate for pleural effusion (sensitivity = 26-53%, specificity = 83-92%, two studies). Treatment was modified in 11 to 54% of the patients (seven studies). POCUS had no significant effect on patient prognosis (two studies). POCUS contributed to patient referrals and transport vectors in 51% (four studies) and 25% (three studies) of patients, respectively. The evidence supports the use of POCUS for managing acute nontraumatic dyspnea in the prehospital setting in terms of feasibility, overall diagnostic contribution, and, particularly, lung ultrasound for acute heart failure diagnosis. Moreover, POCUS seems to have a therapeutic contribution. There is not enough evidence supporting the use of POCUS for pneumonia, pleural effusion, pneumothorax, chronic obstructive pulmonary disease, or asthma exacerbation diagnosis, nor does it support prognostic, patient referral, and transport vector contribution. A high level of evidence is lacking and needed.</p>","PeriodicalId":11893,"journal":{"name":"European Journal of Emergency Medicine","volume":" ","pages":"87-99"},"PeriodicalIF":4.2000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11855997/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/MEJ.0000000000001205","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/3 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"EMERGENCY MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
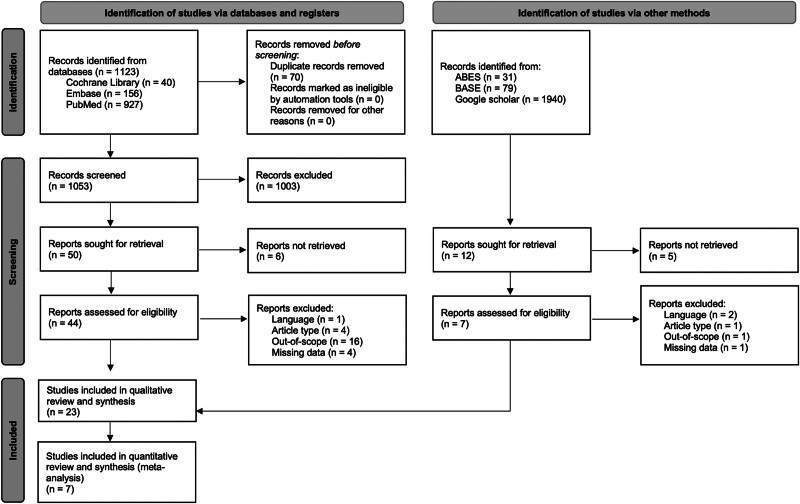
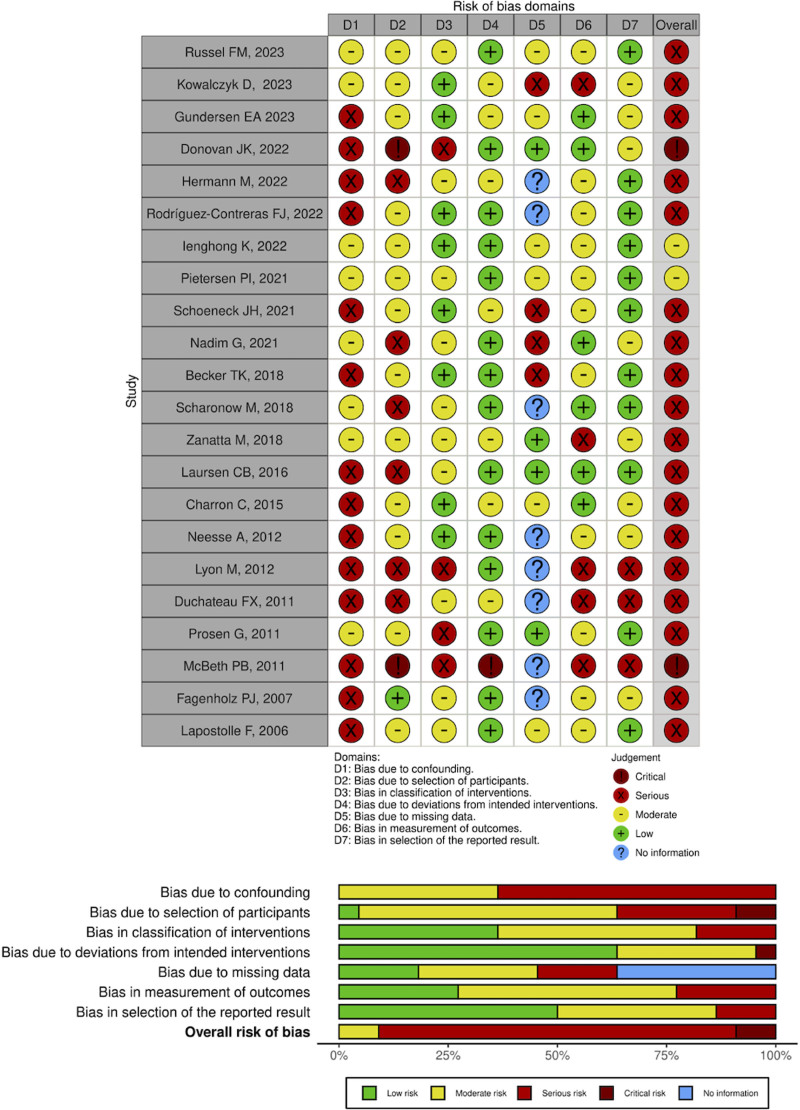
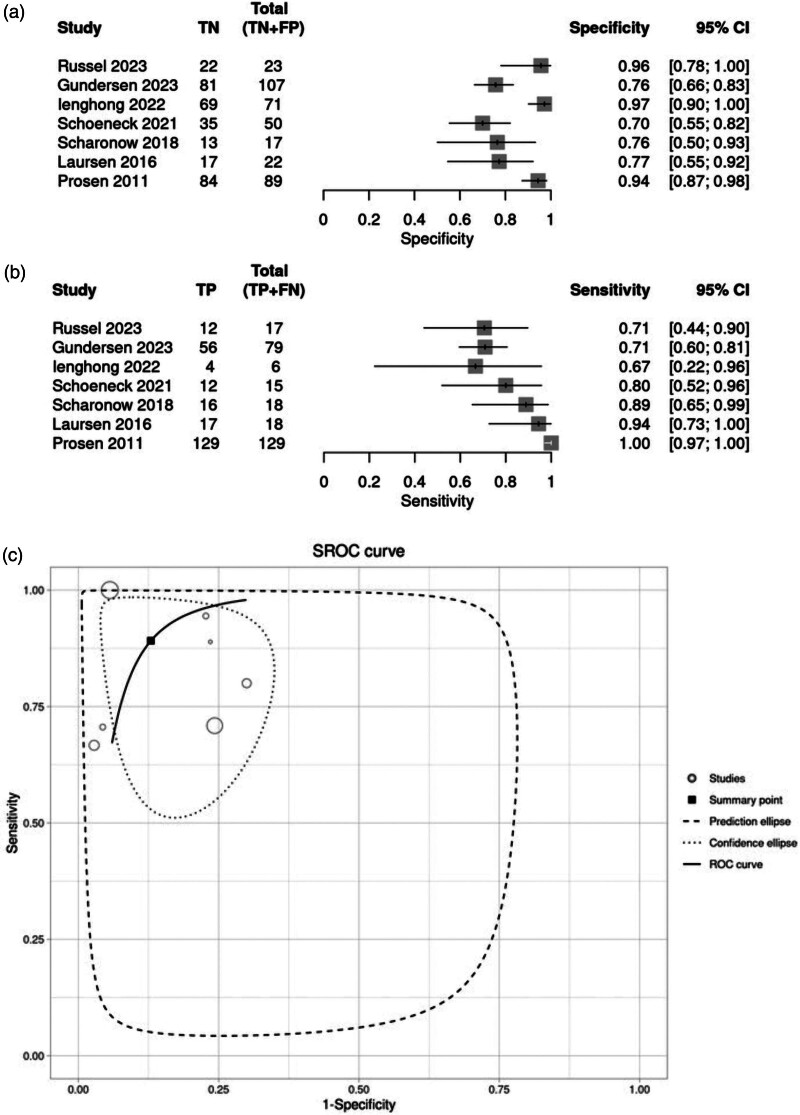
Acute dyspnea is a common symptom whose management is challenging in prehospital settings. Point-of-care ultrasound (POCUS) is increasingly accessible because of device miniaturization. To assess the contribution of POCUS in the prehospital management of patients with acute nontraumatic dyspnea, we performed a systematic review on nontrauma patients of any age managed in the prehospital setting for acute dyspnea and receiving a POCUS examination. We searched seven databases and gray literature for English-language studies published from January 1995 to November 2023. Two independent reviewers completed the study selection, data extraction, and risk of bias assessment. The primary outcome was the assessment of the contribution of POCUS to feasibility, diagnostic, therapeutic, prognosis, patient referral, and transport vector modification. Twenty-three studies were included. The risk of bias assessment identified 3 intermediate-risk, 18 serious-risk, and 2 critical-risk studies. Three studies reported moderate to excellent feasibility for lung POCUS, and three studies reported poor to mediocre feasibility for cardiac POCUS. The median duration of the POCUS examination was less than 5 minutes (six studies). POCUS improved diagnostic identification (seven studies). The diagnostic accuracy of POCUS was excellent for pneumothorax (sensitivity = 100%, specificity = 100%, two studies), very good for acute heart failure (sensitivity = 71-100%, specificity = 72-95%, eight studies), good for pneumonia (sensitivity = 88%, specificity = 59%, one study), and moderate for pleural effusion (sensitivity = 26-53%, specificity = 83-92%, two studies). Treatment was modified in 11 to 54% of the patients (seven studies). POCUS had no significant effect on patient prognosis (two studies). POCUS contributed to patient referrals and transport vectors in 51% (four studies) and 25% (three studies) of patients, respectively. The evidence supports the use of POCUS for managing acute nontraumatic dyspnea in the prehospital setting in terms of feasibility, overall diagnostic contribution, and, particularly, lung ultrasound for acute heart failure diagnosis. Moreover, POCUS seems to have a therapeutic contribution. There is not enough evidence supporting the use of POCUS for pneumonia, pleural effusion, pneumothorax, chronic obstructive pulmonary disease, or asthma exacerbation diagnosis, nor does it support prognostic, patient referral, and transport vector contribution. A high level of evidence is lacking and needed.
期刊介绍:
The European Journal of Emergency Medicine is the official journal of the European Society for Emergency Medicine. It is devoted to serving the European emergency medicine community and to promoting European standards of training, diagnosis and care in this rapidly growing field.
Published bimonthly, the Journal offers original papers on all aspects of acute injury and sudden illness, including: emergency medicine, anaesthesiology, cardiology, disaster medicine, intensive care, internal medicine, orthopaedics, paediatrics, toxicology and trauma care. It addresses issues on the organization of emergency services in hospitals and in the community and examines postgraduate training from European and global perspectives. The Journal also publishes papers focusing on the different models of emergency healthcare delivery in Europe and beyond. With a multidisciplinary approach, the European Journal of Emergency Medicine publishes scientific research, topical reviews, news of meetings and events of interest to the emergency medicine community.
Submitted articles undergo a preliminary review by the editor. Some articles may be returned to authors without further consideration. Those being considered for publication will undergo further assessment and peer-review by the editors and those invited to do so from a reviewer pool.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
