Elisabetta Degasperi , Maria Paola Anolli , Mathias Jachs , Thomas Reiberger , Victor De Ledinghen , Sophie Metivier , Gianpiero D’Offizi , Francesco di Maria , Christoph Schramm , Hartmut Schmidt , Caroline Zöllner , Frank Tacke , Christopher Dietz-Fricke , Heiner Wedemeyer , Margarita Papatheodoridi , George Papatheodoridis , Ivana Carey , Kosh Agarwal , Florian Van Bömmel , Maurizia R. Brunetto , Pietro Lampertico
{"title":"Real-world effectiveness and safety of bulevirtide monotherapy for up to 96 weeks in patients with HDV-related cirrhosis","authors":"Elisabetta Degasperi , Maria Paola Anolli , Mathias Jachs , Thomas Reiberger , Victor De Ledinghen , Sophie Metivier , Gianpiero D’Offizi , Francesco di Maria , Christoph Schramm , Hartmut Schmidt , Caroline Zöllner , Frank Tacke , Christopher Dietz-Fricke , Heiner Wedemeyer , Margarita Papatheodoridi , George Papatheodoridis , Ivana Carey , Kosh Agarwal , Florian Van Bömmel , Maurizia R. Brunetto , Pietro Lampertico","doi":"10.1016/j.jhep.2024.12.044","DOIUrl":null,"url":null,"abstract":"<div><h3>Background & Aims</h3><div>Bulevirtide (BLV) 2 mg/day is EMA approved for the treatment of compensated chronic HDV infection; however, real-world data in large cohorts of patients with cirrhosis are lacking.</div></div><div><h3>Methods</h3><div>Consecutive HDV-infected patients with cirrhosis starting BLV 2 mg/day from September 2019 were included in a European retrospective multicenter real-world study (SAVE-D). Patient characteristics before and during BLV treatment were collected. Virological, biochemical, combined responses, adverse events and liver-related events (hepatocellular carcinoma [HCC], decompensation, liver transplant) were assessed.</div></div><div><h3>Results</h3><div>A total of 244 patients with HDV-related cirrhosis receiving BLV monotherapy for a median of 92 (IQR 71-96) weeks were included: at BLV start, median (IQR) age was 49 (40-58) years and 61% were men; median ALT, LSM and platelet count were 80 (55-130) U/L, 18.3 (13.0-26.3) kPa, and 94 (67-145) x10<sup>3</sup>/mm<sup>3</sup>, respectively; 54% had esophageal varices, 95% Child-Pugh A cirrhosis, and 10% HIV coinfection; 92% were on nucleos(t)ide analogues; median HDV RNA and HBsAg were 5.4 (4.1-6.5) log<sub>10</sub> IU/ml and 3.8 (3.4-4.1) log<sub>10</sub> IU/ml, respectively. At weeks 48 and 96, virological, biochemical and combined responses were observed in 65% and 79%, 61% and 64%, 44% and 54% of patients, respectively. AST, GGT, albumin, IgG and LSM values significantly improved throughout treatment. Serum bile acid levels increased in most patients, but only 10% reported mild and transient pruritus, which was independent of bile acid levels. The week 96 cumulative risks of <em>de novo</em> HCC and decompensation were 3.0% (95% CI 2-6%) and 2.8% (95% CI 1-5%), respectively. Thirteen (5%) patients underwent liver transplantation (n = 11 for HCC, n = 2 for decompensation).</div></div><div><h3>Conclusion</h3><div>BLV 2 mg/day monotherapy for up to 96 weeks was safe and effective in patients with HDV-related cirrhosis. Virological and clinical responses increased over time, while the incidence of liver-related complications was low.</div></div><div><h3>Impact and implications</h3><div>Bulevirtide 2 mg/day is EMA approved for the treatment of compensated chronic hepatitis delta; however, real-world data in large cohorts of patients with cirrhosis are lacking. Bulevirtide 2 mg/day monotherapy for up to 96 weeks was safe and effective (week 96: 79% virological, 64% biochemical and 54% combined response) in a large real-world cohort of patients with HDV-related cirrhosis, including patients with clinically significant portal hypertension. Liver function tests and liver stiffness improved, suggesting a potential clinical benefit in patients with advanced liver disease, while the incidence of <em>de novo</em> liver-related events (hepatocellular carcinoma and decompensation) was low during the 96-week study period.</div></div>","PeriodicalId":15888,"journal":{"name":"Journal of Hepatology","volume":"82 6","pages":"Pages 1012-1022"},"PeriodicalIF":33.0000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepatology","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0168827825000017","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/8 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background & Aims
Bulevirtide (BLV) 2 mg/day is EMA approved for the treatment of compensated chronic HDV infection; however, real-world data in large cohorts of patients with cirrhosis are lacking.
Methods
Consecutive HDV-infected patients with cirrhosis starting BLV 2 mg/day from September 2019 were included in a European retrospective multicenter real-world study (SAVE-D). Patient characteristics before and during BLV treatment were collected. Virological, biochemical, combined responses, adverse events and liver-related events (hepatocellular carcinoma [HCC], decompensation, liver transplant) were assessed.
Results
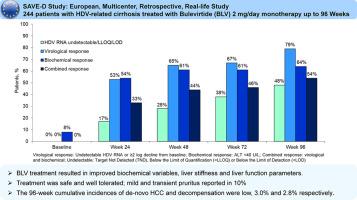
A total of 244 patients with HDV-related cirrhosis receiving BLV monotherapy for a median of 92 (IQR 71-96) weeks were included: at BLV start, median (IQR) age was 49 (40-58) years and 61% were men; median ALT, LSM and platelet count were 80 (55-130) U/L, 18.3 (13.0-26.3) kPa, and 94 (67-145) x103/mm3, respectively; 54% had esophageal varices, 95% Child-Pugh A cirrhosis, and 10% HIV coinfection; 92% were on nucleos(t)ide analogues; median HDV RNA and HBsAg were 5.4 (4.1-6.5) log10 IU/ml and 3.8 (3.4-4.1) log10 IU/ml, respectively. At weeks 48 and 96, virological, biochemical and combined responses were observed in 65% and 79%, 61% and 64%, 44% and 54% of patients, respectively. AST, GGT, albumin, IgG and LSM values significantly improved throughout treatment. Serum bile acid levels increased in most patients, but only 10% reported mild and transient pruritus, which was independent of bile acid levels. The week 96 cumulative risks of de novo HCC and decompensation were 3.0% (95% CI 2-6%) and 2.8% (95% CI 1-5%), respectively. Thirteen (5%) patients underwent liver transplantation (n = 11 for HCC, n = 2 for decompensation).
Conclusion
BLV 2 mg/day monotherapy for up to 96 weeks was safe and effective in patients with HDV-related cirrhosis. Virological and clinical responses increased over time, while the incidence of liver-related complications was low.
Impact and implications
Bulevirtide 2 mg/day is EMA approved for the treatment of compensated chronic hepatitis delta; however, real-world data in large cohorts of patients with cirrhosis are lacking. Bulevirtide 2 mg/day monotherapy for up to 96 weeks was safe and effective (week 96: 79% virological, 64% biochemical and 54% combined response) in a large real-world cohort of patients with HDV-related cirrhosis, including patients with clinically significant portal hypertension. Liver function tests and liver stiffness improved, suggesting a potential clinical benefit in patients with advanced liver disease, while the incidence of de novo liver-related events (hepatocellular carcinoma and decompensation) was low during the 96-week study period.
期刊介绍:
The Journal of Hepatology is the official publication of the European Association for the Study of the Liver (EASL). It is dedicated to presenting clinical and basic research in the field of hepatology through original papers, reviews, case reports, and letters to the Editor. The Journal is published in English and may consider supplements that pass an editorial review.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
