Atacan D. Ertugrul MD , Ary Serpa Neto PhD , Bentley J. Fulcher BPharmSci (Hons) , Anaïs Charles-Nelson PhD , Michael Bailey PhD , Aidan J.C. Burrell PhD , Shannah Anderson BS , Stephen Bernard MD , Jasmin V. Board MPH , Daniel Brodie MD , Heidi Buhr MScMed ClinEpid , D. James Cooper MD , Craig Dicker , Eddy Fan PhD , John F. Fraser PhD , David J. Gattas MMed ClinEpi , Ingrid K. Hopper PhD , Sue Huckson BappSc , Natalie J. Linke BN , Edward Litton PhD , Jing Kong
{"title":"Hospital-level volume in extracorporeal membrane oxygenation cases and death or disability at 6 months","authors":"Atacan D. Ertugrul MD , Ary Serpa Neto PhD , Bentley J. Fulcher BPharmSci (Hons) , Anaïs Charles-Nelson PhD , Michael Bailey PhD , Aidan J.C. Burrell PhD , Shannah Anderson BS , Stephen Bernard MD , Jasmin V. Board MPH , Daniel Brodie MD , Heidi Buhr MScMed ClinEpid , D. James Cooper MD , Craig Dicker , Eddy Fan PhD , John F. Fraser PhD , David J. Gattas MMed ClinEpi , Ingrid K. Hopper PhD , Sue Huckson BappSc , Natalie J. Linke BN , Edward Litton PhD , Jing Kong","doi":"10.1016/j.ccrj.2024.08.006","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><div>Extracorporeal membrane oxygenation (ECMO) is a high-risk procedure with significant morbidity and mortality and there is an uncertain volume-outcome relationship, especially regarding long-term functional outcomes. The aim of this study was to examine the association between ECMO centre volume and long-term death and disability outcomes.</div></div><div><h3>Design, setting, and participants</h3><div>This is a registry-embedded observational cohort study. Patients were included if they were enrolled in the binational ECMO registry (EXCEL). The exclusion criteria included patients on ECMO for heart/lung transplants. Data included demographics, clinical information on their first ECMO run, and six-month outcomes obtained by telephone interview. The primary outcome was death or new disability at six months. A multivariable analysis was conducted using hospitals' annual ECMO volume. High-volume centres were defined as having >30 ECMO cases annually, and analyses were run on ECMO subgroups of veno-venous (VV), veno-arterial (VA), and extracorporeal cardiopulmonary resuscitation (ECPR).</div></div><div><h3>Results</h3><div>Of 1232 patients, 663 patients were cared for on ECMO at high-volume centres and 569 patients at low-volume centres. There was no difference in six-month death or new disability between high- and low-volume ECMO centres in VV-ECMO [OR: 1.09 (0.65–1.83), p = 0.744], VA-ECMO [OR: 1.10 (0.66–1.84), p = 0.708], and ECPR-ECMO [OR: 1.38 (0.37–5.08), p = 0.629]. This finding was persistent in all sensitivity analyses, including exclusion of patients who were transferred between high- and low-volume centres.</div></div><div><h3>Conclusion</h3><div>There was no difference in death or disability at six months between high- and low-volume centres in Australia and New Zealand, possibly due to the current model of coordinated care that includes patient transfers and training between high- and low-volume ECMO centres in our region.</div></div>","PeriodicalId":49215,"journal":{"name":"Critical Care and Resuscitation","volume":"26 4","pages":"Pages 262-270"},"PeriodicalIF":1.7000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11704083/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical Care and Resuscitation","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S1441277224000334","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/22 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
Objective
Extracorporeal membrane oxygenation (ECMO) is a high-risk procedure with significant morbidity and mortality and there is an uncertain volume-outcome relationship, especially regarding long-term functional outcomes. The aim of this study was to examine the association between ECMO centre volume and long-term death and disability outcomes.
Design, setting, and participants
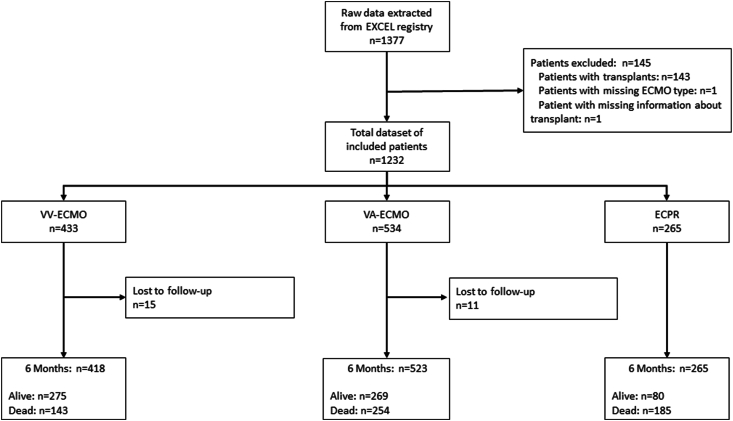
This is a registry-embedded observational cohort study. Patients were included if they were enrolled in the binational ECMO registry (EXCEL). The exclusion criteria included patients on ECMO for heart/lung transplants. Data included demographics, clinical information on their first ECMO run, and six-month outcomes obtained by telephone interview. The primary outcome was death or new disability at six months. A multivariable analysis was conducted using hospitals' annual ECMO volume. High-volume centres were defined as having >30 ECMO cases annually, and analyses were run on ECMO subgroups of veno-venous (VV), veno-arterial (VA), and extracorporeal cardiopulmonary resuscitation (ECPR).
Results
Of 1232 patients, 663 patients were cared for on ECMO at high-volume centres and 569 patients at low-volume centres. There was no difference in six-month death or new disability between high- and low-volume ECMO centres in VV-ECMO [OR: 1.09 (0.65–1.83), p = 0.744], VA-ECMO [OR: 1.10 (0.66–1.84), p = 0.708], and ECPR-ECMO [OR: 1.38 (0.37–5.08), p = 0.629]. This finding was persistent in all sensitivity analyses, including exclusion of patients who were transferred between high- and low-volume centres.
Conclusion
There was no difference in death or disability at six months between high- and low-volume centres in Australia and New Zealand, possibly due to the current model of coordinated care that includes patient transfers and training between high- and low-volume ECMO centres in our region.
期刊介绍:
ritical Care and Resuscitation (CC&R) is the official scientific journal of the College of Intensive Care Medicine (CICM). The Journal is a quarterly publication (ISSN 1441-2772) with original articles of scientific and clinical interest in the specialities of Critical Care, Intensive Care, Anaesthesia, Emergency Medicine and related disciplines.
The Journal is received by all Fellows and trainees, along with an increasing number of subscribers from around the world.
The CC&R Journal currently has an impact factor of 3.3, placing it in 8th position in world critical care journals and in first position in the world outside the USA and Europe.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
