Leon S. Edwards , Milanka Visser , Cecilia Cappelen-Smith , Dennis Cordato , Andrew Bivard , Leonid Churilov , Christopher Blair , James Thomas , Angela Dos Santos , Longting Lin , Chushuang Chen , Carlos Garcia-Esperon , Kenneth Butcher , Tim Kleinig , Phillip MC Choi , Xin Cheng , Qiang Dong , Richard I. Aviv , Mark W. Parsons , on behalf of the INSPIRE Study Group
{"title":"A deep learning approach versus expert clinician panel in the classification of posterior circulation infarction","authors":"Leon S. Edwards , Milanka Visser , Cecilia Cappelen-Smith , Dennis Cordato , Andrew Bivard , Leonid Churilov , Christopher Blair , James Thomas , Angela Dos Santos , Longting Lin , Chushuang Chen , Carlos Garcia-Esperon , Kenneth Butcher , Tim Kleinig , Phillip MC Choi , Xin Cheng , Qiang Dong , Richard I. Aviv , Mark W. Parsons , on behalf of the INSPIRE Study Group","doi":"10.1016/j.nicl.2025.103732","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><div>Posterior circulation infarction (POCI) is common. Imaging techniques such as non-contrast-CT (NCCT) and diffusion-weighted-magnetic-resonance-imaging commonly fail to detect hyperacute POCI. Studies suggest expert inspection of Computed Tomography Perfusion (CTP) improves diagnosis of POCI. In many settings, there is limited access to specialist expertise. Deep-learning has been successfully applied to automate imaging interpretation. This study aimed to develop and validate a deep-learning approach for the classification of POCI using CTP.</div></div><div><h3>Methods</h3><div>Data were analysed from 3541-patients from the International-stroke-perfusion-registry (INSPIRE). All patients with baseline multimodal-CT and follow-up imaging performed at 24–48 h were identified. A cohort of 541-patients was constructed on a 1:3 POCI-to −reference-ratio for model analysis. A 3D-Dense-Convolutional-Network (DenseNet) was trained to classify patients into POCI or non-POCI using CTP-deconvolved-maps. Six-stroke-experts also independently classified patients based upon stepwise access to multimodal CT (mCT) data. DenseNet results were compared against expert clinician results. Model and clinician performance was evaluated using area-under-the-receiver-operating-curve, sensitivity, specificity, accuracy and precision. Clinician agreement was measured with the Fleiss-Kappa-statistic.</div></div><div><h3>Results</h3><div>Best mean clinician diagnostic accuracy, sensitivity and agreement was demonstrated after review of all mCT data (AUC: 0.81, Sensitivity: 0.65, Fleiss-Kappa-statistic: 0.73). There was a spectrum of individual clinician results with an AUC-range of 0.73–0.86. Best DenseNet performance was recorded with an input combination of NCCT and delay-time maps. The DenseNet model was superior to the best mean clinician performance (AUC: 0.87) and was due to enhanced sensitivity (DenseNET: 0.77, Clinician: 0.65). The degree to which the DenseNet model outperformed each clinician ranged and was clinician specific (AUC improvement 0.01–0.14).</div></div><div><h3>Conclusion</h3><div>Comprehensive review of CTP improves diagnostic performance and agreement amongst clinicians. A DenseNet model was superior to best mean clinician performance. The degree of improvement varied by specific clinician. Development of a clinician-DenseNet approach may improve inter-clinician agreement and diagnostic accuracy. This approach may alleviate limited specialist services in resource constrained settings.</div></div>","PeriodicalId":54359,"journal":{"name":"Neuroimage-Clinical","volume":"45 ","pages":"Article 103732"},"PeriodicalIF":3.6000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11786091/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neuroimage-Clinical","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2213158225000026","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/12 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"NEUROIMAGING","Score":null,"Total":0}
引用次数: 0
Abstract
Background
Posterior circulation infarction (POCI) is common. Imaging techniques such as non-contrast-CT (NCCT) and diffusion-weighted-magnetic-resonance-imaging commonly fail to detect hyperacute POCI. Studies suggest expert inspection of Computed Tomography Perfusion (CTP) improves diagnosis of POCI. In many settings, there is limited access to specialist expertise. Deep-learning has been successfully applied to automate imaging interpretation. This study aimed to develop and validate a deep-learning approach for the classification of POCI using CTP.
Methods
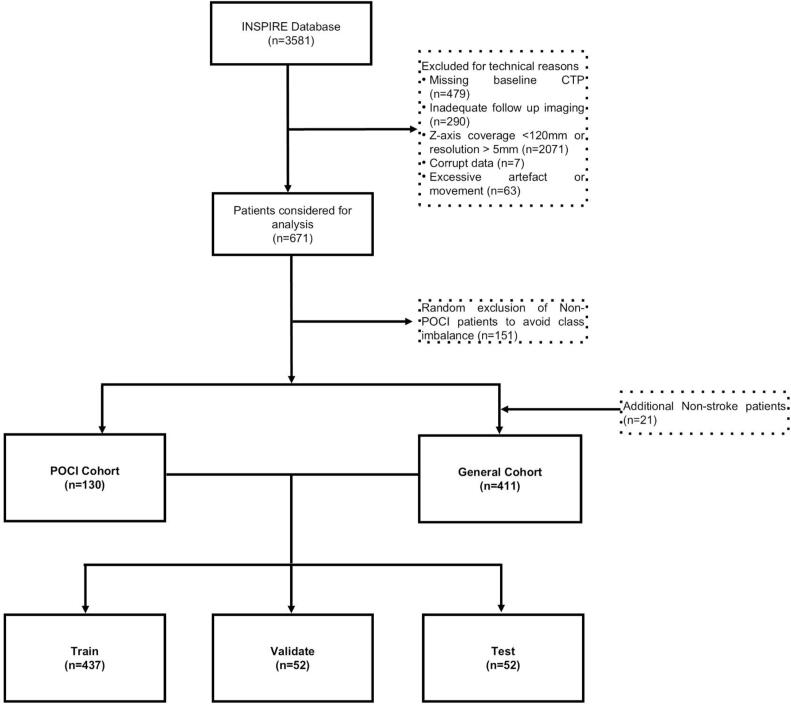
Data were analysed from 3541-patients from the International-stroke-perfusion-registry (INSPIRE). All patients with baseline multimodal-CT and follow-up imaging performed at 24–48 h were identified. A cohort of 541-patients was constructed on a 1:3 POCI-to −reference-ratio for model analysis. A 3D-Dense-Convolutional-Network (DenseNet) was trained to classify patients into POCI or non-POCI using CTP-deconvolved-maps. Six-stroke-experts also independently classified patients based upon stepwise access to multimodal CT (mCT) data. DenseNet results were compared against expert clinician results. Model and clinician performance was evaluated using area-under-the-receiver-operating-curve, sensitivity, specificity, accuracy and precision. Clinician agreement was measured with the Fleiss-Kappa-statistic.
Results
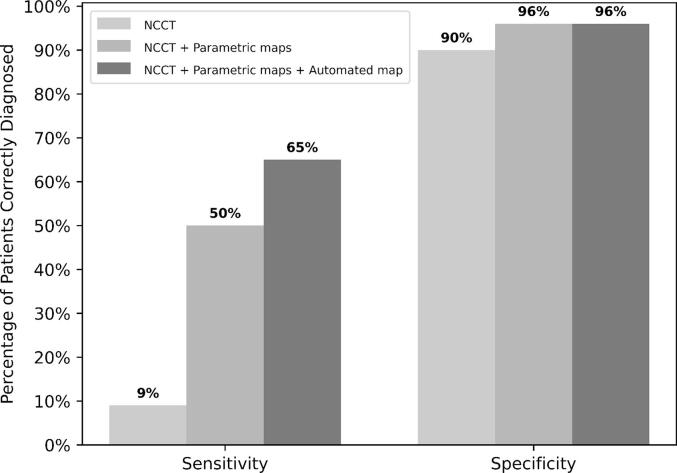
Best mean clinician diagnostic accuracy, sensitivity and agreement was demonstrated after review of all mCT data (AUC: 0.81, Sensitivity: 0.65, Fleiss-Kappa-statistic: 0.73). There was a spectrum of individual clinician results with an AUC-range of 0.73–0.86. Best DenseNet performance was recorded with an input combination of NCCT and delay-time maps. The DenseNet model was superior to the best mean clinician performance (AUC: 0.87) and was due to enhanced sensitivity (DenseNET: 0.77, Clinician: 0.65). The degree to which the DenseNet model outperformed each clinician ranged and was clinician specific (AUC improvement 0.01–0.14).
Conclusion
Comprehensive review of CTP improves diagnostic performance and agreement amongst clinicians. A DenseNet model was superior to best mean clinician performance. The degree of improvement varied by specific clinician. Development of a clinician-DenseNet approach may improve inter-clinician agreement and diagnostic accuracy. This approach may alleviate limited specialist services in resource constrained settings.
期刊介绍:
NeuroImage: Clinical, a journal of diseases, disorders and syndromes involving the Nervous System, provides a vehicle for communicating important advances in the study of abnormal structure-function relationships of the human nervous system based on imaging.
The focus of NeuroImage: Clinical is on defining changes to the brain associated with primary neurologic and psychiatric diseases and disorders of the nervous system as well as behavioral syndromes and developmental conditions. The main criterion for judging papers is the extent of scientific advancement in the understanding of the pathophysiologic mechanisms of diseases and disorders, in identification of functional models that link clinical signs and symptoms with brain function and in the creation of image based tools applicable to a broad range of clinical needs including diagnosis, monitoring and tracking of illness, predicting therapeutic response and development of new treatments. Papers dealing with structure and function in animal models will also be considered if they reveal mechanisms that can be readily translated to human conditions.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
