Anna Trier Heiberg Brix, Tanja Gram Petersen, Tine Nymark, Hagen Schmal, Martin Lindberg-Larsen, Katrine Hass Rubin
{"title":"Increased Mortality After Lower Extremity Amputation in a Danish Nationwide Cohort: The Mediating Role of Postoperative Complications.","authors":"Anna Trier Heiberg Brix, Tanja Gram Petersen, Tine Nymark, Hagen Schmal, Martin Lindberg-Larsen, Katrine Hass Rubin","doi":"10.2147/CLEP.S499167","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Patients who undergo major lower extremity amputation (MLEA) have the highest postoperative mortality among orthopedic patient groups. The comorbidity profile for MLEA patients is often extensive and associated with elevated postoperative mortality. This study primarily aimed to investigate the increased short- and long-term mortality following first and subsequent major lower extremity amputation. Secondarily, to examine the mediation role of post-amputation complications.</p><p><strong>Study design and setting: </strong>With data from the Danish National Patient Registry, 11,695 first-time MLEAs in patients aged ≥50 years were identified between January 1, 2010, and December 31, 2021, along with 58,466 unamputated persons matched 1:5 by year of birth, sex, and region of residence. Mediators were identified through diagnosis codes (ICD-10) present in 6 months following MLEA.</p><p><strong>Results: </strong>The increased mortality following MLEA was highest in the month following MLEA, hazard ratio (HR) 38.7 (95% confidence interval (CI) 30.5-48.9) in women and HR 55.7 (CI 44.3-70.2) in men compared to a matched unamputated cohort. Subsequent amputation resulted in an increased mortality the month after a subsequent amputation (overall HR 3.2 (CI 2.8-3.7) in women and HR 3.2 (CI 2.8-3.6) in men) and almost normalized after the first year. The proportion of the mortality risk that potentially could be reduced by preventing sepsis was 16% (CI 11.7-20.3) for women and 17% (CI 13.4-20.4) for men. For pneumonia, it was 10.5% (CI 7.1-13.9) in women and 14.9% (11.6-18.2) in men.</p><p><strong>Conclusion: </strong>We observed an increased mortality in the month following MLEA, which remained elevated for years compared to the matched unamputated cohort. A subsequent amputation results in increased mortality in the following year, but declined and normalized after the first year. Sepsis and pneumonia arising after the amputation appeared to be important factors that contributed to the increased postoperative mortality.</p>","PeriodicalId":10362,"journal":{"name":"Clinical Epidemiology","volume":"17 ","pages":"27-40"},"PeriodicalIF":3.2000,"publicationDate":"2025-01-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11776520/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Epidemiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2147/CLEP.S499167","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Patients who undergo major lower extremity amputation (MLEA) have the highest postoperative mortality among orthopedic patient groups. The comorbidity profile for MLEA patients is often extensive and associated with elevated postoperative mortality. This study primarily aimed to investigate the increased short- and long-term mortality following first and subsequent major lower extremity amputation. Secondarily, to examine the mediation role of post-amputation complications.
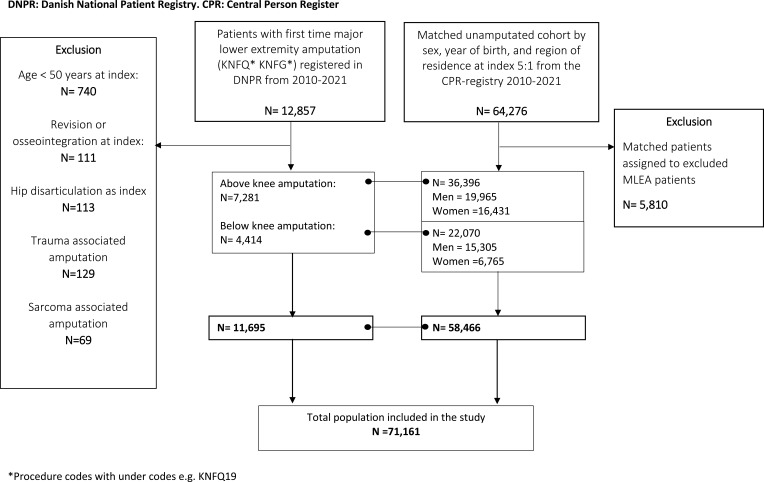
Study design and setting: With data from the Danish National Patient Registry, 11,695 first-time MLEAs in patients aged ≥50 years were identified between January 1, 2010, and December 31, 2021, along with 58,466 unamputated persons matched 1:5 by year of birth, sex, and region of residence. Mediators were identified through diagnosis codes (ICD-10) present in 6 months following MLEA.
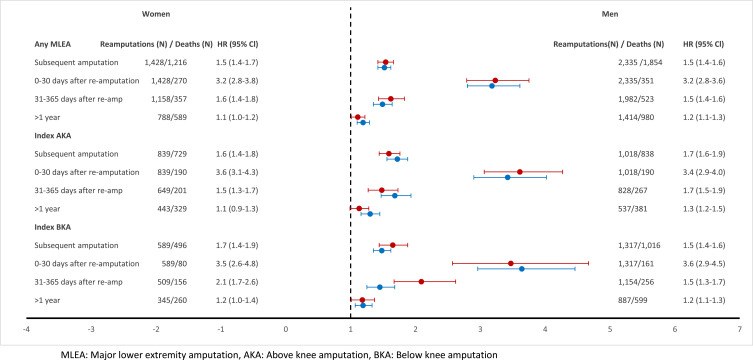
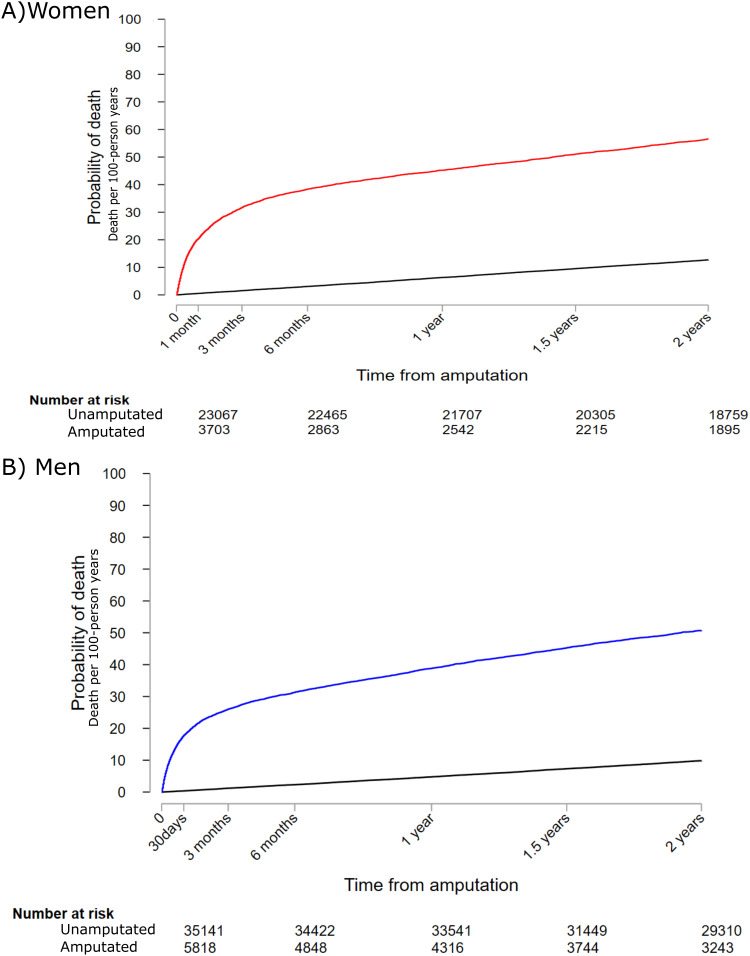
Results: The increased mortality following MLEA was highest in the month following MLEA, hazard ratio (HR) 38.7 (95% confidence interval (CI) 30.5-48.9) in women and HR 55.7 (CI 44.3-70.2) in men compared to a matched unamputated cohort. Subsequent amputation resulted in an increased mortality the month after a subsequent amputation (overall HR 3.2 (CI 2.8-3.7) in women and HR 3.2 (CI 2.8-3.6) in men) and almost normalized after the first year. The proportion of the mortality risk that potentially could be reduced by preventing sepsis was 16% (CI 11.7-20.3) for women and 17% (CI 13.4-20.4) for men. For pneumonia, it was 10.5% (CI 7.1-13.9) in women and 14.9% (11.6-18.2) in men.
Conclusion: We observed an increased mortality in the month following MLEA, which remained elevated for years compared to the matched unamputated cohort. A subsequent amputation results in increased mortality in the following year, but declined and normalized after the first year. Sepsis and pneumonia arising after the amputation appeared to be important factors that contributed to the increased postoperative mortality.
期刊介绍:
Clinical Epidemiology is an international, peer reviewed, open access journal. Clinical Epidemiology focuses on the application of epidemiological principles and questions relating to patients and clinical care in terms of prevention, diagnosis, prognosis, and treatment.
Clinical Epidemiology welcomes papers covering these topics in form of original research and systematic reviews.
Clinical Epidemiology has a special interest in international electronic medical patient records and other routine health care data, especially as applied to safety of medical interventions, clinical utility of diagnostic procedures, understanding short- and long-term clinical course of diseases, clinical epidemiological and biostatistical methods, and systematic reviews.
When considering submission of a paper utilizing publicly-available data, authors should ensure that such studies add significantly to the body of knowledge and that they use appropriate validated methods for identifying health outcomes.
The journal has launched special series describing existing data sources for clinical epidemiology, international health care systems and validation studies of algorithms based on databases and registries.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
