David Kimhy, Luz H Ospina, Melanie Wall, Daniel M Alschuler, Lars F Jarskog, Jacob S Ballon, Joseph McEvoy, Matthew N Bartels, Richard Buchsbaum, Marianne Goodman, Sloane A Miller, T Scott Stroup
{"title":"Telehealth-Based vs In-Person Aerobic Exercise in Individuals With Schizophrenia: Comparative Analysis of Feasibility, Safety, and Efficacy.","authors":"David Kimhy, Luz H Ospina, Melanie Wall, Daniel M Alschuler, Lars F Jarskog, Jacob S Ballon, Joseph McEvoy, Matthew N Bartels, Richard Buchsbaum, Marianne Goodman, Sloane A Miller, T Scott Stroup","doi":"10.2196/68251","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Aerobic exercise (AE) training has been shown to enhance aerobic fitness in people with schizophrenia. Traditionally, such training has been administered in person at gyms or other communal exercise spaces. However, following the advent of the COVID-19 pandemic, many clinics transitioned their services to telehealth-based delivery. Yet, at present, there is scarce information about the feasibility, safety, and efficacy of telehealth-based AE in this population.</p><p><strong>Objective: </strong>To examine the feasibility, safety, and efficacy of trainer-led, at-home, telehealth-based AE in individuals with schizophrenia.</p><p><strong>Methods: </strong>We analyzed data from the AE arm (n=37) of a single-blind, randomized clinical trial examining the impact of a 12-week AE intervention in people with schizophrenia. Following the onset of the COVID-19 pandemic, the AE trial intervention transitioned from in-person to at-home, telehealth-based delivery of AE, with the training frequency and duration remaining identical. We compared the feasibility, safety, and efficacy of the delivery of trainer-led AE training among participants undergoing in-person (pre-COVID-19; n=23) versus at-home telehealth AE (post-COVID-19; n=14).</p><p><strong>Results: </strong>The telehealth and in-person participants attended a similar number of exercise sessions across the 12-week interventions (26.8, SD 10.2 vs 26.1, SD 9.7, respectively; P=.84) and had similar number of weeks with at least 1 exercise session (10.4, SD 3.4 vs 10.6, SD 3.1, respectively; P=.79). The telehealth-based AE was associated with a significantly lower drop-out rate (telehealth: 0/14, 0%; in-person: 7/23, 30.4%; P=.04). There were no significant group differences in total time spent exercising (telehealth: 1246, SD 686 min; in-person: 1494, SD 580 min; P=.28); however, over the 12-week intervention, the telehealth group had a significantly lower proportion of session-time exercising at or above target intensity (telehealth: 33.3%, SD 21.4%; in-person: 63.5%, SD 16.3%; P<.001). There were no AE-related serious adverse events associated with either AE delivery format. Similarly, there were no significant differences in the percentage of participants experiencing minor or moderate adverse events, such as muscle soreness, joint pain, blisters, or dyspnea (telehealth: 3/14, 21%; in-person: 5/19, 26%; P>.99) or in the percentage of weeks per participant with at least 1 exercise-related adverse event (telehealth: 31%, SD 33%; in-person: 40%, SD 33%; P=.44). There were no significant differences between the telehealth versus in-person groups regarding changes in aerobic fitness as indexed by maximum oxygen consumption (VO2max; P=.27).</p><p><strong>Conclusions: </strong>Our findings provide preliminary support for the delivery of telehealth-based AE for individuals with schizophrenia. Our results indicate that in-home telehealth-based AE is feasible and safe in this population, although when available, in-person AE appears preferable given the opportunity for social interactions and the higher intensity of exercises. We discuss the findings' clinical implications, specifically within the context of the COVID-19 pandemic, as well as review potential challenges for the implementation of telehealth-based AE among people with schizophrenia.</p>","PeriodicalId":48616,"journal":{"name":"Jmir Mental Health","volume":"12 ","pages":"e68251"},"PeriodicalIF":5.8000,"publicationDate":"2025-02-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11844875/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Jmir Mental Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2196/68251","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Aerobic exercise (AE) training has been shown to enhance aerobic fitness in people with schizophrenia. Traditionally, such training has been administered in person at gyms or other communal exercise spaces. However, following the advent of the COVID-19 pandemic, many clinics transitioned their services to telehealth-based delivery. Yet, at present, there is scarce information about the feasibility, safety, and efficacy of telehealth-based AE in this population.
Objective: To examine the feasibility, safety, and efficacy of trainer-led, at-home, telehealth-based AE in individuals with schizophrenia.
Methods: We analyzed data from the AE arm (n=37) of a single-blind, randomized clinical trial examining the impact of a 12-week AE intervention in people with schizophrenia. Following the onset of the COVID-19 pandemic, the AE trial intervention transitioned from in-person to at-home, telehealth-based delivery of AE, with the training frequency and duration remaining identical. We compared the feasibility, safety, and efficacy of the delivery of trainer-led AE training among participants undergoing in-person (pre-COVID-19; n=23) versus at-home telehealth AE (post-COVID-19; n=14).
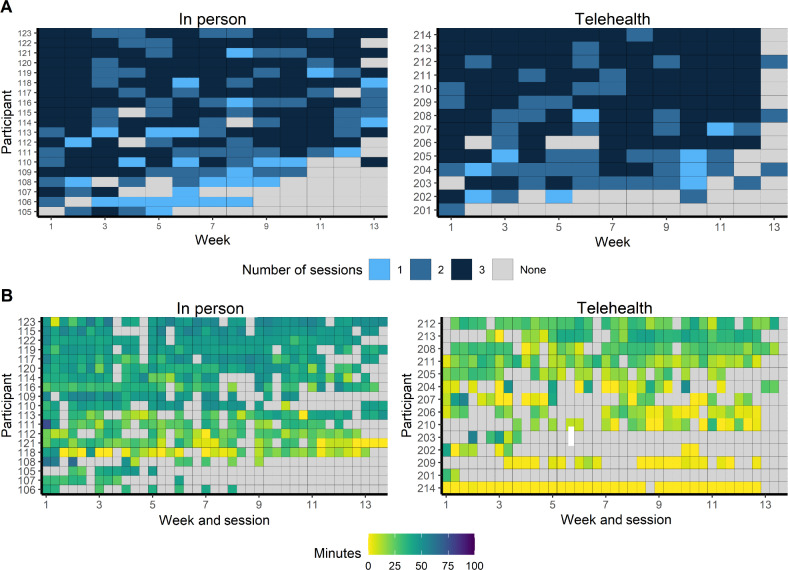
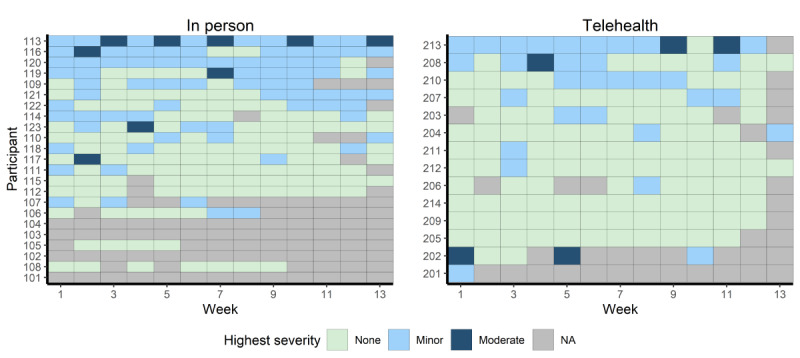
Results: The telehealth and in-person participants attended a similar number of exercise sessions across the 12-week interventions (26.8, SD 10.2 vs 26.1, SD 9.7, respectively; P=.84) and had similar number of weeks with at least 1 exercise session (10.4, SD 3.4 vs 10.6, SD 3.1, respectively; P=.79). The telehealth-based AE was associated with a significantly lower drop-out rate (telehealth: 0/14, 0%; in-person: 7/23, 30.4%; P=.04). There were no significant group differences in total time spent exercising (telehealth: 1246, SD 686 min; in-person: 1494, SD 580 min; P=.28); however, over the 12-week intervention, the telehealth group had a significantly lower proportion of session-time exercising at or above target intensity (telehealth: 33.3%, SD 21.4%; in-person: 63.5%, SD 16.3%; P<.001). There were no AE-related serious adverse events associated with either AE delivery format. Similarly, there were no significant differences in the percentage of participants experiencing minor or moderate adverse events, such as muscle soreness, joint pain, blisters, or dyspnea (telehealth: 3/14, 21%; in-person: 5/19, 26%; P>.99) or in the percentage of weeks per participant with at least 1 exercise-related adverse event (telehealth: 31%, SD 33%; in-person: 40%, SD 33%; P=.44). There were no significant differences between the telehealth versus in-person groups regarding changes in aerobic fitness as indexed by maximum oxygen consumption (VO2max; P=.27).
Conclusions: Our findings provide preliminary support for the delivery of telehealth-based AE for individuals with schizophrenia. Our results indicate that in-home telehealth-based AE is feasible and safe in this population, although when available, in-person AE appears preferable given the opportunity for social interactions and the higher intensity of exercises. We discuss the findings' clinical implications, specifically within the context of the COVID-19 pandemic, as well as review potential challenges for the implementation of telehealth-based AE among people with schizophrenia.
期刊介绍:
JMIR Mental Health (JMH, ISSN 2368-7959) is a PubMed-indexed, peer-reviewed sister journal of JMIR, the leading eHealth journal (Impact Factor 2016: 5.175).
JMIR Mental Health focusses on digital health and Internet interventions, technologies and electronic innovations (software and hardware) for mental health, addictions, online counselling and behaviour change. This includes formative evaluation and system descriptions, theoretical papers, review papers, viewpoint/vision papers, and rigorous evaluations.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
