Mobile Electronic Patient-Reported Outcomes and Interactive Support During Breast and Prostate Cancer Treatment: Health Economic Evaluation From Two Randomized Controlled Trials.
Marie-Therése Crafoord, Joakim Ekstrand, Kay Sundberg, Marie I Nilsson, Maria Fjell, Ann Langius-Eklöf
{"title":"Mobile Electronic Patient-Reported Outcomes and Interactive Support During Breast and Prostate Cancer Treatment: Health Economic Evaluation From Two Randomized Controlled Trials.","authors":"Marie-Therése Crafoord, Joakim Ekstrand, Kay Sundberg, Marie I Nilsson, Maria Fjell, Ann Langius-Eklöf","doi":"10.2196/53539","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Digital interventions for supportive care during cancer treatment incorporating electronic patient-reported outcomes (ePROs) can enhance early detection of symptoms and facilitate timely symptom management. However, economic evaluations are needed.</p><p><strong>Objective: </strong>This study aims to conduct a cost-utility analysis of an app for ePRO and interactive support from the perspective of the payer (Region Stockholm Health Care Organization) and to explore its impact on patient health care utilization and costs.</p><p><strong>Methods: </strong>Two open-label randomized controlled trials (RCTs) were conducted, including patients undergoing neoadjuvant chemotherapy for breast cancer (B-RCT; N=149) and radiotherapy for prostate cancer (P-RCT; N=150), recruited from oncology clinics at 2 university hospitals in Stockholm, Sweden. EORTC QLQ-C30 scores were mapped to EQ-5D-3L to calculate quality-adjusted life years (QALYs). Intervention and implementation costs and health care costs, obtained from an administrative database, were used to calculate incremental cost-effectiveness ratios (ICERs) in 3 ways: including all health care costs (ICERa), excluding nonacute health care costs (ICERb), and excluding health care costs altogether (ICERc). Nonparametric bootstrapping was used to explore ICER uncertainty. Health care costs were analyzed by classifying them as disease-related or acute.</p><p><strong>Results: </strong>In both RCT intervention groups, fewer QALYs were lost compared with the control group (P<.001). In the B-RCT, the mean intervention cost was €92 (SD €2; €1=US $1.03). The mean cost for the intervention and all health care was €36,882 (SD €1032) in the intervention group and €35,427 (SD €959) in the control group (P<.001), with an ICERa of €202,368 (95% CI €152,008-€252,728). The mean cost for the intervention and acute health care was €3585 (SD €480) in the intervention group and €3235 (SD €494) in the control group (P<.001). ICERb was €49,903 (95% CI €37,049-€62,758) and ICERc was €13,213 (95% CI €11,145-€15,281); 22 out of 74 (30%) intervention group patients and 24 out of 75 (32%) of the control group patients required acute inpatient care for fever. In the P-RCT, the mean intervention cost was €43 (SD €0.2). The mean cost for the intervention and all health care was €3419 (SD €739) in the intervention group and €3537 (SD €689) in the control group (P<.001), with an ICERa of -€1,092,136 (95% CI -€3,274,774 to €1,090,502). The mean cost for the intervention and acute health care was €1219 (SD €593) in the intervention group and €802 (SD €281) in the control group (P<.001). ICERb was €745,987 (95% CI -€247,317 to €1,739,292) and ICERc was €13,118 (95% CI -68,468 to €94,704). As many as 10 out of the 75 (13%) intervention group patients had acute inpatient care, with the most common symptom being dyspnea, while 9 out of the 75 (12%) control group patients had acute inpatient care, with the most common symptom being urinary tract infection.</p><p><strong>Conclusions: </strong>ePRO and interactive support via an app generated a small improvement in QALYs at a low intervention cost and may be cost-effective, depending on the costs considered. Considerable variability in patient health care costs introduced uncertainty around the estimates, preventing a robust determination of cost-effectiveness. Larger studies examining cost-effectiveness from a societal perspective are needed. The study provides valuable insights into acute health care utilization during cancer treatment.</p><p><strong>Trial registration: </strong>ClinicalTrials.gov NCT02479607; https://clinicaltrials.gov/ct2/show/NCT02479607, ClinicalTrials.gov NCT02477137; https://clinicaltrials.gov/ct2/show/NCT02477137.</p><p><strong>International registered report identifier (irrid): </strong>RR2-10.1186/s12885-017-3450-y.</p>","PeriodicalId":45538,"journal":{"name":"JMIR Cancer","volume":"11 ","pages":"e53539"},"PeriodicalIF":2.7000,"publicationDate":"2025-03-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11937708/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR Cancer","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/53539","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Digital interventions for supportive care during cancer treatment incorporating electronic patient-reported outcomes (ePROs) can enhance early detection of symptoms and facilitate timely symptom management. However, economic evaluations are needed.
Objective: This study aims to conduct a cost-utility analysis of an app for ePRO and interactive support from the perspective of the payer (Region Stockholm Health Care Organization) and to explore its impact on patient health care utilization and costs.
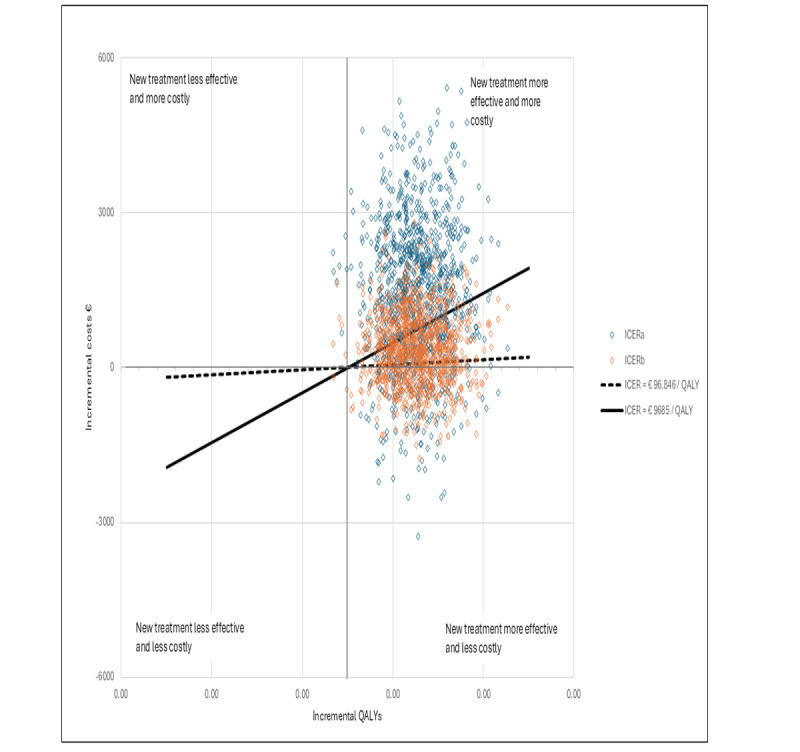
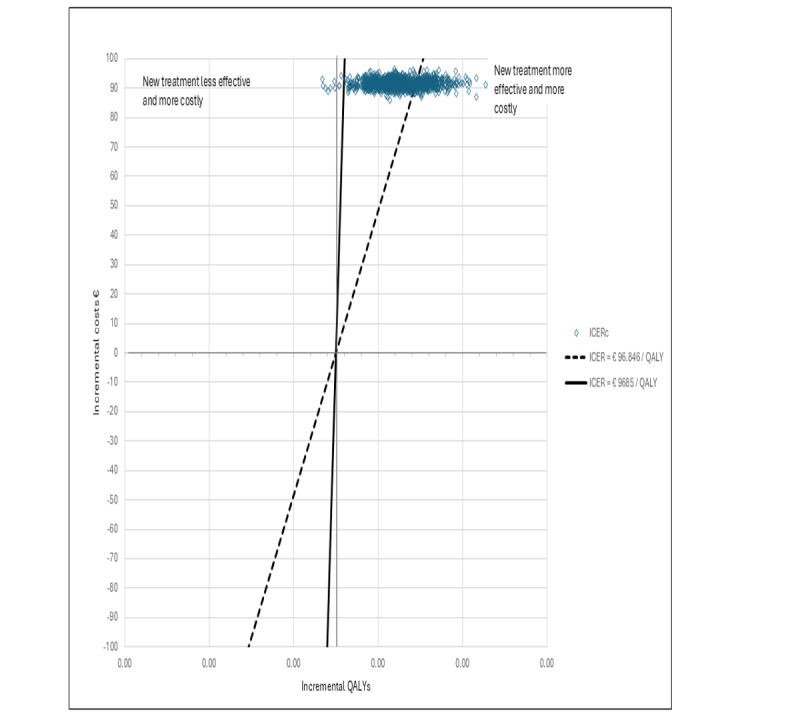
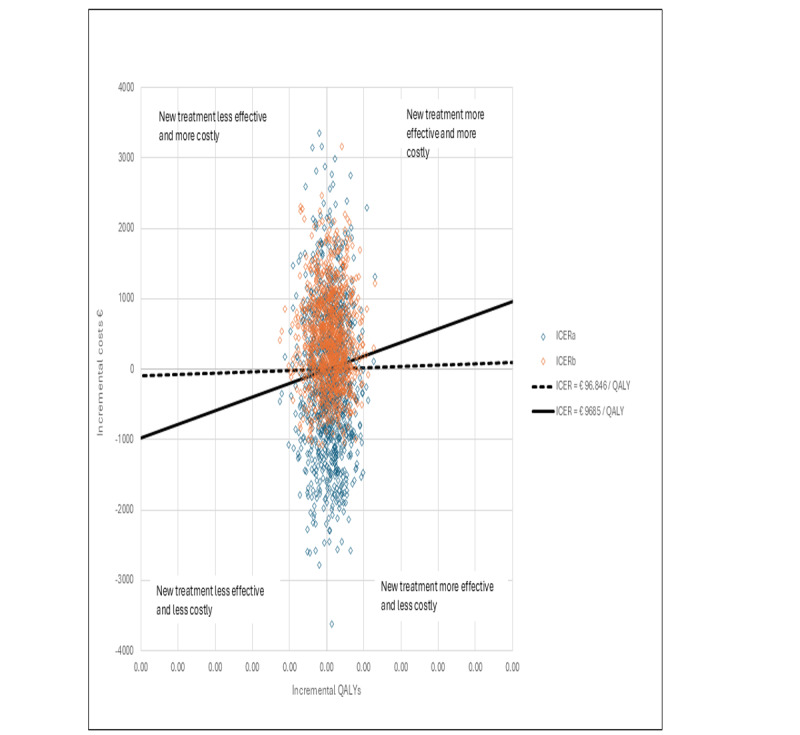
Methods: Two open-label randomized controlled trials (RCTs) were conducted, including patients undergoing neoadjuvant chemotherapy for breast cancer (B-RCT; N=149) and radiotherapy for prostate cancer (P-RCT; N=150), recruited from oncology clinics at 2 university hospitals in Stockholm, Sweden. EORTC QLQ-C30 scores were mapped to EQ-5D-3L to calculate quality-adjusted life years (QALYs). Intervention and implementation costs and health care costs, obtained from an administrative database, were used to calculate incremental cost-effectiveness ratios (ICERs) in 3 ways: including all health care costs (ICERa), excluding nonacute health care costs (ICERb), and excluding health care costs altogether (ICERc). Nonparametric bootstrapping was used to explore ICER uncertainty. Health care costs were analyzed by classifying them as disease-related or acute.
Results: In both RCT intervention groups, fewer QALYs were lost compared with the control group (P<.001). In the B-RCT, the mean intervention cost was €92 (SD €2; €1=US $1.03). The mean cost for the intervention and all health care was €36,882 (SD €1032) in the intervention group and €35,427 (SD €959) in the control group (P<.001), with an ICERa of €202,368 (95% CI €152,008-€252,728). The mean cost for the intervention and acute health care was €3585 (SD €480) in the intervention group and €3235 (SD €494) in the control group (P<.001). ICERb was €49,903 (95% CI €37,049-€62,758) and ICERc was €13,213 (95% CI €11,145-€15,281); 22 out of 74 (30%) intervention group patients and 24 out of 75 (32%) of the control group patients required acute inpatient care for fever. In the P-RCT, the mean intervention cost was €43 (SD €0.2). The mean cost for the intervention and all health care was €3419 (SD €739) in the intervention group and €3537 (SD €689) in the control group (P<.001), with an ICERa of -€1,092,136 (95% CI -€3,274,774 to €1,090,502). The mean cost for the intervention and acute health care was €1219 (SD €593) in the intervention group and €802 (SD €281) in the control group (P<.001). ICERb was €745,987 (95% CI -€247,317 to €1,739,292) and ICERc was €13,118 (95% CI -68,468 to €94,704). As many as 10 out of the 75 (13%) intervention group patients had acute inpatient care, with the most common symptom being dyspnea, while 9 out of the 75 (12%) control group patients had acute inpatient care, with the most common symptom being urinary tract infection.
Conclusions: ePRO and interactive support via an app generated a small improvement in QALYs at a low intervention cost and may be cost-effective, depending on the costs considered. Considerable variability in patient health care costs introduced uncertainty around the estimates, preventing a robust determination of cost-effectiveness. Larger studies examining cost-effectiveness from a societal perspective are needed. The study provides valuable insights into acute health care utilization during cancer treatment.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
