Shengjia Xu, Niloofar Fouladi Nashta, Yi Chen, Julie Zissimopoulos
{"title":"Association of Dementia Severity at Diagnosis With Health Care Utilization and Costs Around the Time of Incident Diagnosis.","authors":"Shengjia Xu, Niloofar Fouladi Nashta, Yi Chen, Julie Zissimopoulos","doi":"10.1093/geroni/igaf005","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>This study provides the first analysis of heterogeneity in health care use and costs by level of dementia symptom severity around the time of incident dementia diagnosis for a population-representative sample of older Americans.</p><p><strong>Research design and methods: </strong>We used the Aging, Demographics, and Memory Study (ADAMS), the Health Retirement Study (HRS), and traditional Medicare (TM) claims. We modeled dementia severity measured by the Clinical Dementia Rating scale for ADAMS respondents and applied parameter estimates to HRS respondents older than 70 years who had a claims-based incident dementia diagnosis in 2000-2016. We used claims-based measures of health care costs and use and quantified levels in the quarters before, at, and after a dementia diagnosis. We reported separate results for groups of persons diagnosed at mild, moderate, and severe stages of dementia.</p><p><strong>Results: </strong>Health care use and costs increased a quarter before dementia diagnosis and increased most significantly in the quarter of diagnosis. Both use and costs declined thereafter but remained elevated relative to prediagnosis. This general pattern was consistent for persons diagnosed at different stages of dementia. Acute care costs were similar across dementia severity categories throughout the period, whereas outpatient use and costs were consistently higher among persons diagnosed at mild stage disease.</p><p><strong>Discussion and implications: </strong>Findings from this study provide new insights on how heterogeneity of dementia severity at diagnosis is associated with health care use and costs. Under the current system of care in TM, early dementia diagnosis may not substantially reduce health care use and spending around the time of dementia diagnosis.</p>","PeriodicalId":13596,"journal":{"name":"Innovation in Aging","volume":"9 3","pages":"igaf005"},"PeriodicalIF":4.3000,"publicationDate":"2025-01-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11911999/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Innovation in Aging","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/geroni/igaf005","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background and objectives: This study provides the first analysis of heterogeneity in health care use and costs by level of dementia symptom severity around the time of incident dementia diagnosis for a population-representative sample of older Americans.
Research design and methods: We used the Aging, Demographics, and Memory Study (ADAMS), the Health Retirement Study (HRS), and traditional Medicare (TM) claims. We modeled dementia severity measured by the Clinical Dementia Rating scale for ADAMS respondents and applied parameter estimates to HRS respondents older than 70 years who had a claims-based incident dementia diagnosis in 2000-2016. We used claims-based measures of health care costs and use and quantified levels in the quarters before, at, and after a dementia diagnosis. We reported separate results for groups of persons diagnosed at mild, moderate, and severe stages of dementia.
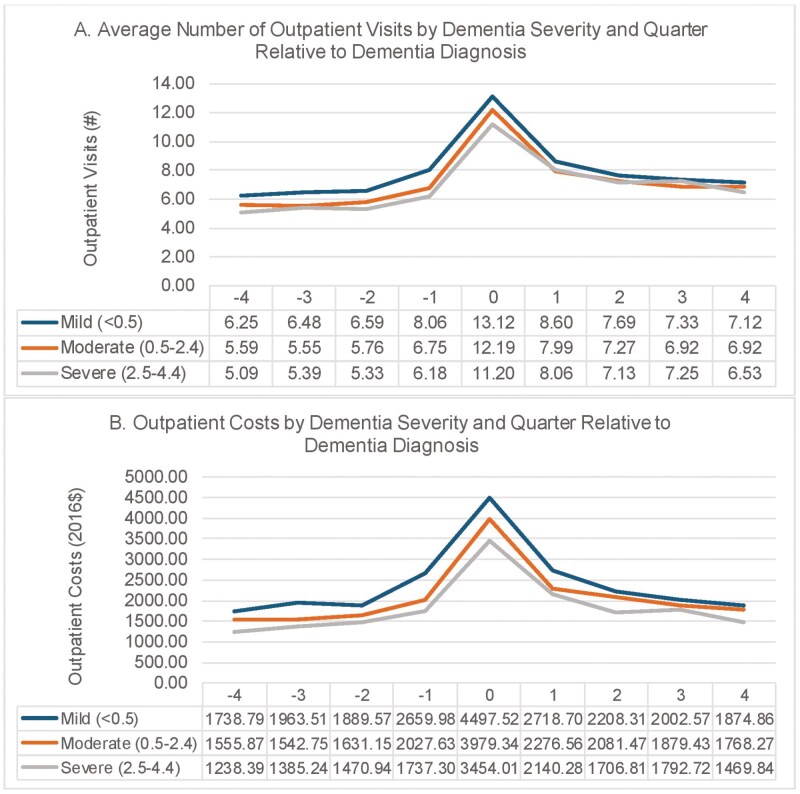
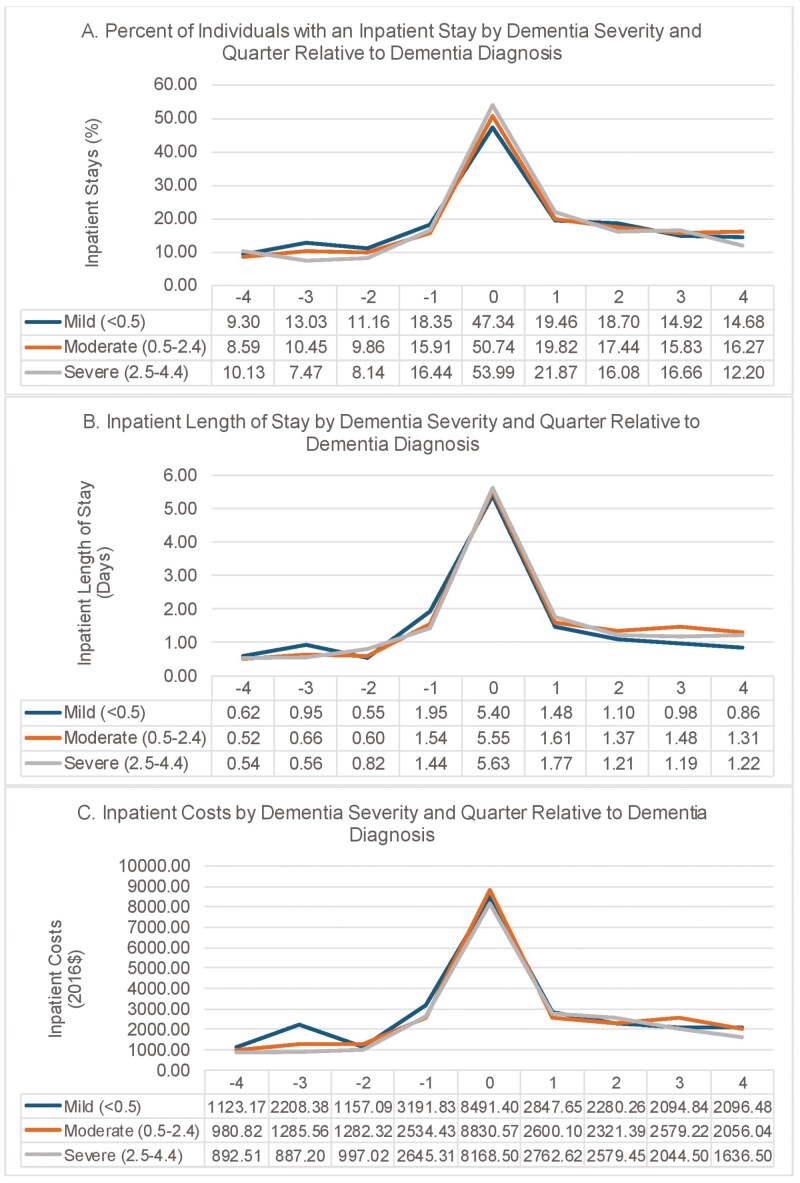
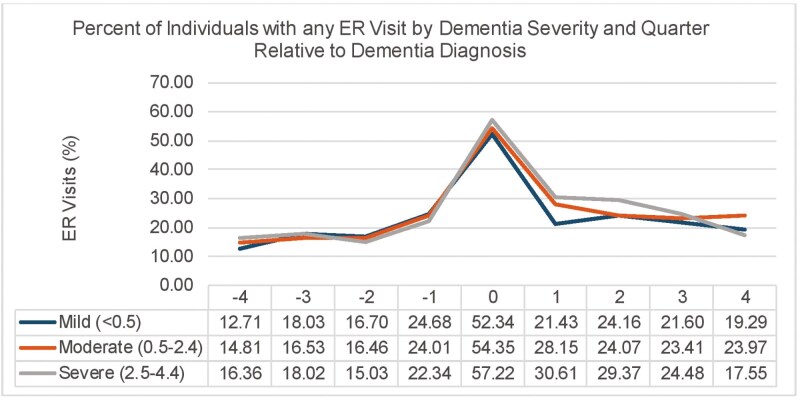
Results: Health care use and costs increased a quarter before dementia diagnosis and increased most significantly in the quarter of diagnosis. Both use and costs declined thereafter but remained elevated relative to prediagnosis. This general pattern was consistent for persons diagnosed at different stages of dementia. Acute care costs were similar across dementia severity categories throughout the period, whereas outpatient use and costs were consistently higher among persons diagnosed at mild stage disease.
Discussion and implications: Findings from this study provide new insights on how heterogeneity of dementia severity at diagnosis is associated with health care use and costs. Under the current system of care in TM, early dementia diagnosis may not substantially reduce health care use and spending around the time of dementia diagnosis.
期刊介绍:
Innovation in Aging, an interdisciplinary Open Access journal of the Gerontological Society of America (GSA), is dedicated to publishing innovative, conceptually robust, and methodologically rigorous research focused on aging and the life course. The journal aims to present studies with the potential to significantly enhance the health, functionality, and overall well-being of older adults by translating scientific insights into practical applications. Research published in the journal spans a variety of settings, including community, clinical, and laboratory contexts, with a clear emphasis on issues that are directly pertinent to aging and the dynamics of life over time. The content of the journal mirrors the diverse research interests of GSA members and encompasses a range of study types. These include the validation of new conceptual or theoretical models, assessments of factors impacting the health and well-being of older adults, evaluations of interventions and policies, the implementation of groundbreaking research methodologies, interdisciplinary research that adapts concepts and methods from other fields to aging studies, and the use of modeling and simulations to understand factors and processes influencing aging outcomes. The journal welcomes contributions from scholars across various disciplines, such as technology, engineering, architecture, economics, business, law, political science, public policy, education, public health, social and psychological sciences, biomedical and health sciences, and the humanities and arts, reflecting a holistic approach to advancing knowledge in gerontology.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
