Ali Zedan, Essam Elshiekh, Mohamed I Omar, Mohamad Raafat, Salah M Khallaf, Haisam Atta, Marwa T Hussien
{"title":"Laparoscopic versus Open Complete Mesocolic Excision for Right Colon Cancer.","authors":"Ali Zedan, Essam Elshiekh, Mohamed I Omar, Mohamad Raafat, Salah M Khallaf, Haisam Atta, Marwa T Hussien","doi":"10.1155/2021/8859879","DOIUrl":null,"url":null,"abstract":"Results The mean operative time was significantly longer in the LCME group than that in the OCME group with less mean intraoperative blood loss. Conversion was required in 4 patients (8.3%) in the LCME group. The use of laparoscopy increased the number of harvested lymph nodes compared to the open approach (39.81 ± 16.74 vs. 32.65 ± 12.28, respectively, P=0.010). The laparoscopic approach was associated with a shorter time interval to first flatus as well as shorter time interval to liquid and normal diet after surgery. The postoperative hospital stay was significantly shorter in the LCME group. The complication rate was slightly lower in the LCME (14.7%) than in the OCME group (27.2%) (P=0.252). The 3-year OS in the LCME group was similar to that in OCME (78.2% vs. 63.2%, respectively, P value = 0.423). The three-year DFS in the laparoscopic group was higher (74.5%) than the open group (60.0%), but did not reach statistical significance (P value = 0.266). Conclusions In conclusion, laparoscopic CME right hemicolectomy is a technically feasible and safe procedure if surgeon expertise is present. LCME has long-term oncologic outcomes (recurrence and survival) comparable to open surgery for management of patients with stage II or III colon cancer.","PeriodicalId":45960,"journal":{"name":"International Journal of Surgical Oncology","volume":"2021 ","pages":"8859879"},"PeriodicalIF":1.6000,"publicationDate":"2021-02-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7872753/pdf/","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Surgical Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2021/8859879","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 8
Abstract
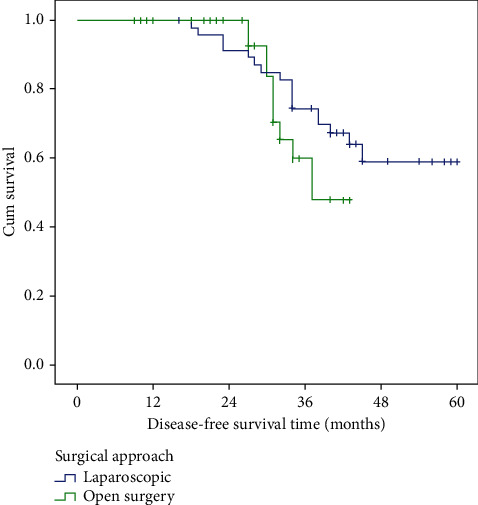
Results The mean operative time was significantly longer in the LCME group than that in the OCME group with less mean intraoperative blood loss. Conversion was required in 4 patients (8.3%) in the LCME group. The use of laparoscopy increased the number of harvested lymph nodes compared to the open approach (39.81 ± 16.74 vs. 32.65 ± 12.28, respectively, P=0.010). The laparoscopic approach was associated with a shorter time interval to first flatus as well as shorter time interval to liquid and normal diet after surgery. The postoperative hospital stay was significantly shorter in the LCME group. The complication rate was slightly lower in the LCME (14.7%) than in the OCME group (27.2%) (P=0.252). The 3-year OS in the LCME group was similar to that in OCME (78.2% vs. 63.2%, respectively, P value = 0.423). The three-year DFS in the laparoscopic group was higher (74.5%) than the open group (60.0%), but did not reach statistical significance (P value = 0.266). Conclusions In conclusion, laparoscopic CME right hemicolectomy is a technically feasible and safe procedure if surgeon expertise is present. LCME has long-term oncologic outcomes (recurrence and survival) comparable to open surgery for management of patients with stage II or III colon cancer.
期刊介绍:
International Journal of Surgical Oncology is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies in all areas of surgical oncology.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
