Stephanie Riley, Kimberly Tam, Wai-Yee Tse, Andrew Connor, Yinghui Wei
{"title":"在英国移植人群中存在半竞争事件的肾脏供者风险指数的外部验证。","authors":"Stephanie Riley, Kimberly Tam, Wai-Yee Tse, Andrew Connor, Yinghui Wei","doi":"10.1186/s41512-023-00159-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Transplantation represents the optimal treatment for many patients with end-stage kidney disease. When a donor kidney is available to a waitlisted patient, clinicians responsible for the care of the potential recipient must make the decision to accept or decline the offer based upon complex and variable information about the donor, the recipient and the transplant process. A clinical prediction model may be able to support clinicians in their decision-making. The Kidney Donor Risk Index (KDRI) was developed in the United States to predict graft failure following kidney transplantation. The survival process following transplantation consists of semi-competing events where death precludes graft failure, but not vice-versa.</p><p><strong>Methods: </strong>We externally validated the KDRI in the UK kidney transplant population and assessed whether validation under a semi-competing risks framework impacted predictive performance. Additionally, we explored whether the KDRI requires updating. We included 20,035 adult recipients of first, deceased donor, single, kidney-only transplants between January 1, 2004, and December 31, 2018, collected by the UK Transplant Registry and held by NHS Blood and Transplant. The outcomes of interest were 1- and 5-year graft failure following transplantation. In light of the semi-competing events, recipient death was handled in two ways: censoring patients at the time of death and modelling death as a competing event. Cox proportional hazard models were used to validate the KDRI when censoring graft failure by death, and cause-specific Cox models were used to account for death as a competing event.</p><p><strong>Results: </strong>The KDRI underestimated event probabilities for those at higher risk of graft failure. For 5-year graft failure, discrimination was poorer in the semi-competing risks model (0.625, 95% CI 0.611 to 0.640;0.611, 95% CI 0.597 to 0.625), but predictions were more accurate (Brier score 0.117, 95% CI 0.112 to 0.121; 0.114, 95% CI 0.109 to 0.118). Calibration plots were similar regardless of whether the death was modelled as a competing event or not. Updating the KDRI worsened calibration, but marginally improved discrimination.</p><p><strong>Conclusions: </strong>Predictive performance for 1-year graft failure was similar between death-censored and competing event graft failure, but differences appeared when predicting 5-year graft failure. The updated index did not have superior performance and we conclude that updating the KDRI in the present form is not required.</p>","PeriodicalId":72800,"journal":{"name":"Diagnostic and prognostic research","volume":"7 1","pages":"20"},"PeriodicalIF":2.6000,"publicationDate":"2023-11-21","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10662562/pdf/","citationCount":"0","resultStr":"{\"title\":\"An external validation of the Kidney Donor Risk Index in the UK transplant population in the presence of semi-competing events.\",\"authors\":\"Stephanie Riley, Kimberly Tam, Wai-Yee Tse, Andrew Connor, Yinghui Wei\",\"doi\":\"10.1186/s41512-023-00159-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Transplantation represents the optimal treatment for many patients with end-stage kidney disease. When a donor kidney is available to a waitlisted patient, clinicians responsible for the care of the potential recipient must make the decision to accept or decline the offer based upon complex and variable information about the donor, the recipient and the transplant process. A clinical prediction model may be able to support clinicians in their decision-making. The Kidney Donor Risk Index (KDRI) was developed in the United States to predict graft failure following kidney transplantation. The survival process following transplantation consists of semi-competing events where death precludes graft failure, but not vice-versa.</p><p><strong>Methods: </strong>We externally validated the KDRI in the UK kidney transplant population and assessed whether validation under a semi-competing risks framework impacted predictive performance. Additionally, we explored whether the KDRI requires updating. We included 20,035 adult recipients of first, deceased donor, single, kidney-only transplants between January 1, 2004, and December 31, 2018, collected by the UK Transplant Registry and held by NHS Blood and Transplant. The outcomes of interest were 1- and 5-year graft failure following transplantation. In light of the semi-competing events, recipient death was handled in two ways: censoring patients at the time of death and modelling death as a competing event. Cox proportional hazard models were used to validate the KDRI when censoring graft failure by death, and cause-specific Cox models were used to account for death as a competing event.</p><p><strong>Results: </strong>The KDRI underestimated event probabilities for those at higher risk of graft failure. For 5-year graft failure, discrimination was poorer in the semi-competing risks model (0.625, 95% CI 0.611 to 0.640;0.611, 95% CI 0.597 to 0.625), but predictions were more accurate (Brier score 0.117, 95% CI 0.112 to 0.121; 0.114, 95% CI 0.109 to 0.118). Calibration plots were similar regardless of whether the death was modelled as a competing event or not. Updating the KDRI worsened calibration, but marginally improved discrimination.</p><p><strong>Conclusions: </strong>Predictive performance for 1-year graft failure was similar between death-censored and competing event graft failure, but differences appeared when predicting 5-year graft failure. The updated index did not have superior performance and we conclude that updating the KDRI in the present form is not required.</p>\",\"PeriodicalId\":72800,\"journal\":{\"name\":\"Diagnostic and prognostic research\",\"volume\":\"7 1\",\"pages\":\"20\"},\"PeriodicalIF\":2.6000,\"publicationDate\":\"2023-11-21\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10662562/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Diagnostic and prognostic research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41512-023-00159-9\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Diagnostic and prognostic research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41512-023-00159-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
摘要
背景:移植是许多终末期肾病患者的最佳治疗方法。当一个等待名单的病人可以得到一个供体肾脏时,负责照顾潜在受体的临床医生必须根据关于供体、受体和移植过程的复杂和可变的信息做出接受或拒绝这个提议的决定。临床预测模型可以支持临床医生的决策。肾供者风险指数(KDRI)是在美国开发的,用于预测肾移植后移植物衰竭。移植后的生存过程包括半竞争事件,其中死亡排除移植物衰竭,但反之亦然。方法:我们在英国肾移植人群中对KDRI进行了外部验证,并评估了在半竞争风险框架下的验证是否会影响预测性能。此外,我们探讨了KDRI是否需要更新。我们纳入了2004年1月1日至2018年12月31日期间,由英国移植登记中心收集并由NHS血液和移植中心保存的20,035名首次、已故捐赠者、单肾移植的成年受者。关注的结果是移植后1年和5年的移植物衰竭。鉴于半竞争性事件,接受者死亡的处理有两种方式:在死亡时对患者进行审查,并将死亡模拟为竞争性事件。在审查死亡导致的移植物衰竭时,使用Cox比例风险模型来验证KDRI,并使用病因特异性Cox模型来解释死亡作为竞争事件。结果:KDRI低估了移植物衰竭高危人群的事件概率。对于5年移植物衰竭,半竞争风险模型的鉴别性较差(0.625,95% CI 0.611 ~ 0.640;0.611, 95% CI 0.597 ~ 0.625),但预测更准确(Brier评分0.117,95% CI 0.112 ~ 0.121;0.114, 95% CI 0.109 ~ 0.118)。无论死亡是否被建模为竞争事件,校准图都是相似的。更新KDRI恶化了校准,但略微改善了识别。结论:对1年移植物衰竭的预测性能在死亡审查和竞争事件移植物衰竭之间相似,但在预测5年移植物衰竭时出现差异。更新后的指数没有更好的表现,我们得出结论,更新目前形式的KDRI是没有必要的。
An external validation of the Kidney Donor Risk Index in the UK transplant population in the presence of semi-competing events.
Background: Transplantation represents the optimal treatment for many patients with end-stage kidney disease. When a donor kidney is available to a waitlisted patient, clinicians responsible for the care of the potential recipient must make the decision to accept or decline the offer based upon complex and variable information about the donor, the recipient and the transplant process. A clinical prediction model may be able to support clinicians in their decision-making. The Kidney Donor Risk Index (KDRI) was developed in the United States to predict graft failure following kidney transplantation. The survival process following transplantation consists of semi-competing events where death precludes graft failure, but not vice-versa.
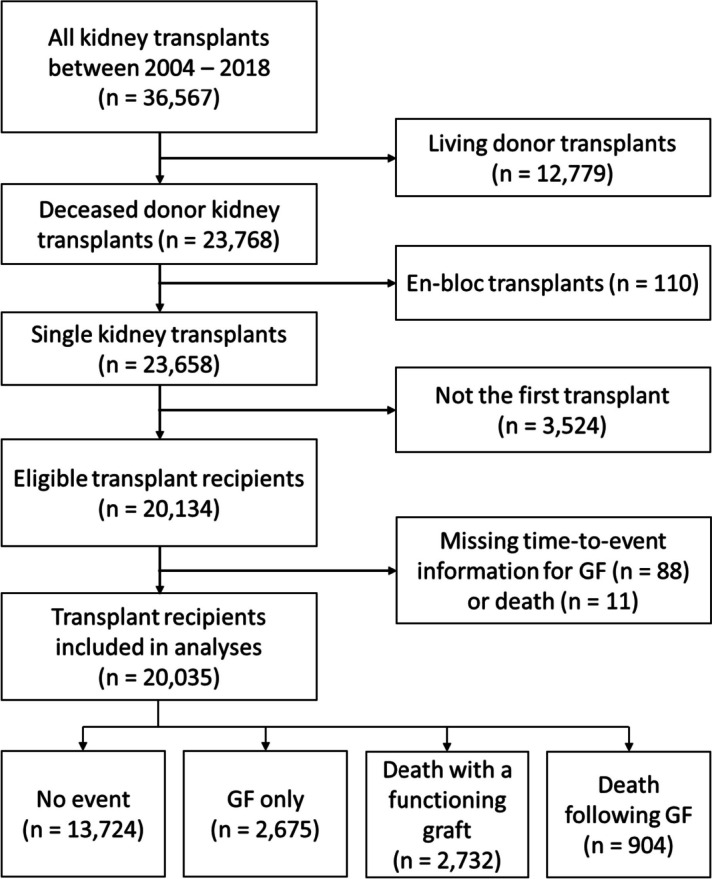
Methods: We externally validated the KDRI in the UK kidney transplant population and assessed whether validation under a semi-competing risks framework impacted predictive performance. Additionally, we explored whether the KDRI requires updating. We included 20,035 adult recipients of first, deceased donor, single, kidney-only transplants between January 1, 2004, and December 31, 2018, collected by the UK Transplant Registry and held by NHS Blood and Transplant. The outcomes of interest were 1- and 5-year graft failure following transplantation. In light of the semi-competing events, recipient death was handled in two ways: censoring patients at the time of death and modelling death as a competing event. Cox proportional hazard models were used to validate the KDRI when censoring graft failure by death, and cause-specific Cox models were used to account for death as a competing event.
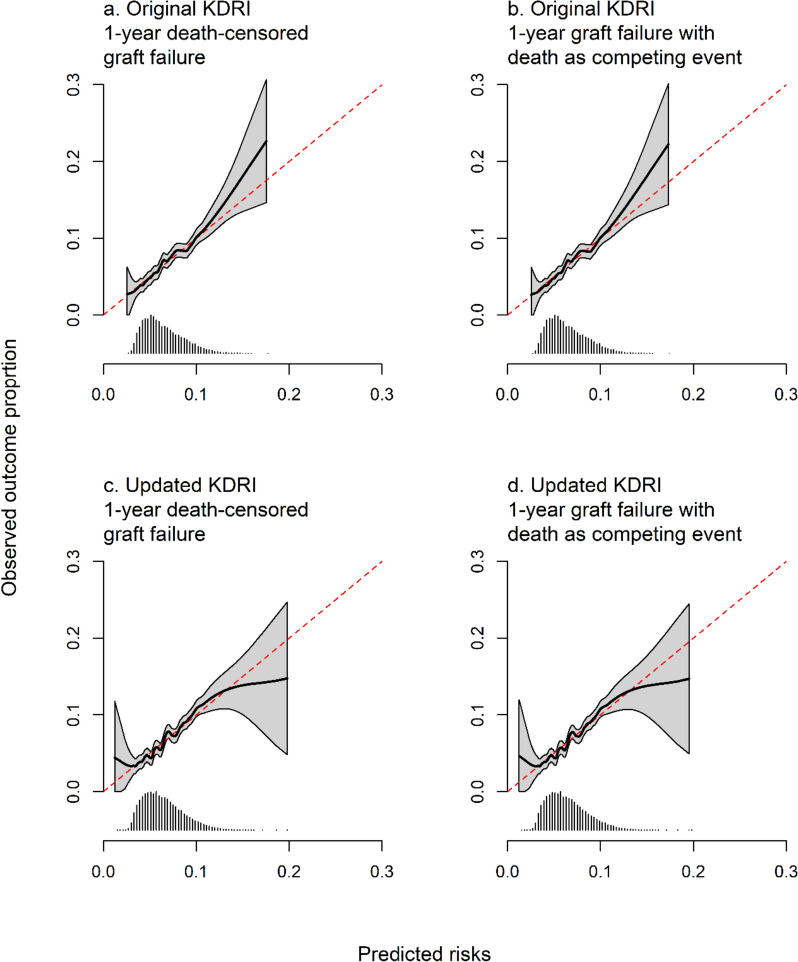
Results: The KDRI underestimated event probabilities for those at higher risk of graft failure. For 5-year graft failure, discrimination was poorer in the semi-competing risks model (0.625, 95% CI 0.611 to 0.640;0.611, 95% CI 0.597 to 0.625), but predictions were more accurate (Brier score 0.117, 95% CI 0.112 to 0.121; 0.114, 95% CI 0.109 to 0.118). Calibration plots were similar regardless of whether the death was modelled as a competing event or not. Updating the KDRI worsened calibration, but marginally improved discrimination.
Conclusions: Predictive performance for 1-year graft failure was similar between death-censored and competing event graft failure, but differences appeared when predicting 5-year graft failure. The updated index did not have superior performance and we conclude that updating the KDRI in the present form is not required.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
