{"title":"利用支架牵引器:在内镜逆行性阑尾炎治疗中处理阑尾孔狭窄的新技术。","authors":"Zhiqian Chen, Junxiu Li, Xianhui Zeng","doi":"10.1111/den.14793","DOIUrl":null,"url":null,"abstract":"<p>A 52-year-old woman suffering the migration of abdominal pain to right lower quadrant, nausea, and diarrhea sought medical attention in the emergency department. Laboratory investigations revealed a white blood cell count of 12.7 × 10<sup>9</sup>/L, and ultrasound imaging demonstrated an appendiceal diameter of 12 mm without evidence of perforation and tumor (Fig. 1). Acute uncomplicated appendicitis (AUA), the primary indication for endoscopic retrograde appendicitis therapy (ERAT),<span><sup>1</sup></span> was diagnosed. Therefore, she was referred to our department following informed consent.</p><p>During the ERAT, purulent material emanated from the appendix (Fig. 2a). Repeated attempts to place a contrast catheter (5.5F) through the guidewire failed (Video S1). The stenosis of the appendiceal orifice was considered. We skillfully used a Soehendra stent retriever (Wilson-Cook Medical, Inc., Winston-Salem, NC, USA) (Fig. 2b) to gradually dilate the orifice, facilitating the smooth passage of the contrast catheter into the appendiceal lumen (Fig. 2c, Video S1). After flushing, no significant stenosis was visualized by iohexol radiography (Fig. 2d). A 5F × 5 cm stent was then placed (Fig. 2e). Follow-up coloscopy on 2-month postoperative showed the stent was dislodged, and no abnormality was seen in the appendiceal opening (Fig. 2f).</p><p>Appendiceal lumen obstruction stands as the predominant etiology of acute appendicitis.<span><sup>2</sup></span> The constriction of the appendiceal orifice may contribute to this obstruction. However, the successful treatment of appendicitis attributed to appendiceal orifice stenosis by ERAT has been rarely reported, because stenosis is less likely to occur in AUA,<span><sup>3</sup></span> and surgery is an alternative remedy in instances where ERAT encounters challenges in placing guidewires and contrast catheters.<span><sup>4</sup></span> The electrosurgical incision of the appendiceal orifice to alleviate stenosis has been reported,<span><sup>5</sup></span> albeit with a heightened risk of perforation. The Soehendra stent retriever not only advanced along the guidewire but also functioned as a dilator by means of rotation, offering a safer alternative to mitigate the risk of perforation associated with electrosurgical incision.</p><p>Authors declare no conflict of interest for this article.</p><p>Crosswise Project of West China Fourth Hospital, Sichuan University (No. 01-186) and Crosswise Project of Sichuan University (No. 22H0415).</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":null,"pages":null},"PeriodicalIF":5.0000,"publicationDate":"2024-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14793","citationCount":"0","resultStr":"{\"title\":\"Utilizing a stent retriever: Novel technique for the management of appendiceal orifice stenosis during endoscopic retrograde appendicitis therapy\",\"authors\":\"Zhiqian Chen, Junxiu Li, Xianhui Zeng\",\"doi\":\"10.1111/den.14793\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>A 52-year-old woman suffering the migration of abdominal pain to right lower quadrant, nausea, and diarrhea sought medical attention in the emergency department. Laboratory investigations revealed a white blood cell count of 12.7 × 10<sup>9</sup>/L, and ultrasound imaging demonstrated an appendiceal diameter of 12 mm without evidence of perforation and tumor (Fig. 1). Acute uncomplicated appendicitis (AUA), the primary indication for endoscopic retrograde appendicitis therapy (ERAT),<span><sup>1</sup></span> was diagnosed. Therefore, she was referred to our department following informed consent.</p><p>During the ERAT, purulent material emanated from the appendix (Fig. 2a). Repeated attempts to place a contrast catheter (5.5F) through the guidewire failed (Video S1). The stenosis of the appendiceal orifice was considered. We skillfully used a Soehendra stent retriever (Wilson-Cook Medical, Inc., Winston-Salem, NC, USA) (Fig. 2b) to gradually dilate the orifice, facilitating the smooth passage of the contrast catheter into the appendiceal lumen (Fig. 2c, Video S1). After flushing, no significant stenosis was visualized by iohexol radiography (Fig. 2d). A 5F × 5 cm stent was then placed (Fig. 2e). Follow-up coloscopy on 2-month postoperative showed the stent was dislodged, and no abnormality was seen in the appendiceal opening (Fig. 2f).</p><p>Appendiceal lumen obstruction stands as the predominant etiology of acute appendicitis.<span><sup>2</sup></span> The constriction of the appendiceal orifice may contribute to this obstruction. However, the successful treatment of appendicitis attributed to appendiceal orifice stenosis by ERAT has been rarely reported, because stenosis is less likely to occur in AUA,<span><sup>3</sup></span> and surgery is an alternative remedy in instances where ERAT encounters challenges in placing guidewires and contrast catheters.<span><sup>4</sup></span> The electrosurgical incision of the appendiceal orifice to alleviate stenosis has been reported,<span><sup>5</sup></span> albeit with a heightened risk of perforation. The Soehendra stent retriever not only advanced along the guidewire but also functioned as a dilator by means of rotation, offering a safer alternative to mitigate the risk of perforation associated with electrosurgical incision.</p><p>Authors declare no conflict of interest for this article.</p><p>Crosswise Project of West China Fourth Hospital, Sichuan University (No. 01-186) and Crosswise Project of Sichuan University (No. 22H0415).</p>\",\"PeriodicalId\":159,\"journal\":{\"name\":\"Digestive Endoscopy\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":5.0000,\"publicationDate\":\"2024-04-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14793\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Digestive Endoscopy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/den.14793\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14793","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Utilizing a stent retriever: Novel technique for the management of appendiceal orifice stenosis during endoscopic retrograde appendicitis therapy
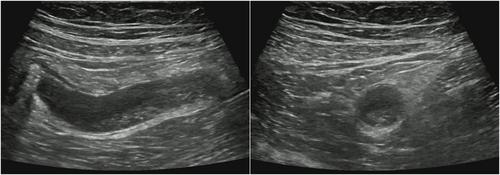
A 52-year-old woman suffering the migration of abdominal pain to right lower quadrant, nausea, and diarrhea sought medical attention in the emergency department. Laboratory investigations revealed a white blood cell count of 12.7 × 109/L, and ultrasound imaging demonstrated an appendiceal diameter of 12 mm without evidence of perforation and tumor (Fig. 1). Acute uncomplicated appendicitis (AUA), the primary indication for endoscopic retrograde appendicitis therapy (ERAT),1 was diagnosed. Therefore, she was referred to our department following informed consent.
During the ERAT, purulent material emanated from the appendix (Fig. 2a). Repeated attempts to place a contrast catheter (5.5F) through the guidewire failed (Video S1). The stenosis of the appendiceal orifice was considered. We skillfully used a Soehendra stent retriever (Wilson-Cook Medical, Inc., Winston-Salem, NC, USA) (Fig. 2b) to gradually dilate the orifice, facilitating the smooth passage of the contrast catheter into the appendiceal lumen (Fig. 2c, Video S1). After flushing, no significant stenosis was visualized by iohexol radiography (Fig. 2d). A 5F × 5 cm stent was then placed (Fig. 2e). Follow-up coloscopy on 2-month postoperative showed the stent was dislodged, and no abnormality was seen in the appendiceal opening (Fig. 2f).
Appendiceal lumen obstruction stands as the predominant etiology of acute appendicitis.2 The constriction of the appendiceal orifice may contribute to this obstruction. However, the successful treatment of appendicitis attributed to appendiceal orifice stenosis by ERAT has been rarely reported, because stenosis is less likely to occur in AUA,3 and surgery is an alternative remedy in instances where ERAT encounters challenges in placing guidewires and contrast catheters.4 The electrosurgical incision of the appendiceal orifice to alleviate stenosis has been reported,5 albeit with a heightened risk of perforation. The Soehendra stent retriever not only advanced along the guidewire but also functioned as a dilator by means of rotation, offering a safer alternative to mitigate the risk of perforation associated with electrosurgical incision.
Authors declare no conflict of interest for this article.
Crosswise Project of West China Fourth Hospital, Sichuan University (No. 01-186) and Crosswise Project of Sichuan University (No. 22H0415).
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
