Valentino Dammassa, Costanza Natalia Julia Colombo, Massimo Erba, Fabio Ciarrocchi, Michele Pagani, Susanna Price, Francesco Mojoli, Guido Tavazzi
{"title":"COVID-19 相关急性呼吸窘迫综合征右心室功能的超声心动图评估:收缩-舒张相互作用的重要性。","authors":"Valentino Dammassa, Costanza Natalia Julia Colombo, Massimo Erba, Fabio Ciarrocchi, Michele Pagani, Susanna Price, Francesco Mojoli, Guido Tavazzi","doi":"10.1186/s13089-024-00366-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The cardiac manifestations of COVID-19 have been described in patients with acute respiratory distress syndrome (ARDS) admitted to intensive care unit (ICU). The presence and impact of right ventricular (RV) diastolic function and performance has not been studied in this population yet. We describe the prevalence of RV diastolic dysfunction, assessed by the pulmonary valve pre-ejection A wave (PV A wave), and the RV systo-diastolic interaction, using the RV total isovolumic time (t-IVT), in COVID-19 ARDS.</p><p><strong>Results: </strong>Prospective observational study enrolling patients with moderate to severe COVID-19 ARDS admitted to ICU who underwent a transthoracic echocardiogram within 24 h of ICU admission and at least a second one during the ICU stay. Respiratory, hemodynamic and biochemistry parameters were collected. 163 patients (age 61.0 ± 9.3 years, 72% males) were enrolled. 36 patients (22.1%) had RV dysfunction, 45 (27.1%) LV systolic dysfunction. 73 patients (44.7%) had PV A wave. The RV t-IVT correlated with TAPSE at ICU admission (p < 0.002; r - 0.61), presence of PV A wave (p < 0.001; r 0.78), peak inspiratory pressure (PIP) (p < 0.001; r 0.42), PEEP (p < 0.001; r 0.68), dynamic driving pressure (DDP) (p < 0.001; r 0.58), and PaO<sub>2</sub>/FiO<sub>2</sub> ratio (p < 0.01; r - 0.35). The presence of PV A wave was associated with higher PIP (p < 0.001; r 0.45), higher PEEP (p < 0.001; r 0.56), higher DDP (p < 0.01, r 0.51), and lower PaO<sub>2</sub>/FiO<sub>2</sub> ratio (p < 0.001; r - 0.49).</p><p><strong>Conclusions: </strong>RV t-IVT and the presence of PV A wave are non-invasive means to describe a significant RV diastolic dysfunction and may be consider descriptive signs of RV performance in COVID-19 ARDS.</p>","PeriodicalId":36911,"journal":{"name":"Ultrasound Journal","volume":"16 1","pages":"26"},"PeriodicalIF":3.6000,"publicationDate":"2024-05-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11076422/pdf/","citationCount":"0","resultStr":"{\"title\":\"Echocardiographic assessment of right ventricular performance in COVID-19 related acute respiratory distress syndrome: the importance of systo-diastolic interaction.\",\"authors\":\"Valentino Dammassa, Costanza Natalia Julia Colombo, Massimo Erba, Fabio Ciarrocchi, Michele Pagani, Susanna Price, Francesco Mojoli, Guido Tavazzi\",\"doi\":\"10.1186/s13089-024-00366-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The cardiac manifestations of COVID-19 have been described in patients with acute respiratory distress syndrome (ARDS) admitted to intensive care unit (ICU). The presence and impact of right ventricular (RV) diastolic function and performance has not been studied in this population yet. We describe the prevalence of RV diastolic dysfunction, assessed by the pulmonary valve pre-ejection A wave (PV A wave), and the RV systo-diastolic interaction, using the RV total isovolumic time (t-IVT), in COVID-19 ARDS.</p><p><strong>Results: </strong>Prospective observational study enrolling patients with moderate to severe COVID-19 ARDS admitted to ICU who underwent a transthoracic echocardiogram within 24 h of ICU admission and at least a second one during the ICU stay. Respiratory, hemodynamic and biochemistry parameters were collected. 163 patients (age 61.0 ± 9.3 years, 72% males) were enrolled. 36 patients (22.1%) had RV dysfunction, 45 (27.1%) LV systolic dysfunction. 73 patients (44.7%) had PV A wave. The RV t-IVT correlated with TAPSE at ICU admission (p < 0.002; r - 0.61), presence of PV A wave (p < 0.001; r 0.78), peak inspiratory pressure (PIP) (p < 0.001; r 0.42), PEEP (p < 0.001; r 0.68), dynamic driving pressure (DDP) (p < 0.001; r 0.58), and PaO<sub>2</sub>/FiO<sub>2</sub> ratio (p < 0.01; r - 0.35). The presence of PV A wave was associated with higher PIP (p < 0.001; r 0.45), higher PEEP (p < 0.001; r 0.56), higher DDP (p < 0.01, r 0.51), and lower PaO<sub>2</sub>/FiO<sub>2</sub> ratio (p < 0.001; r - 0.49).</p><p><strong>Conclusions: </strong>RV t-IVT and the presence of PV A wave are non-invasive means to describe a significant RV diastolic dysfunction and may be consider descriptive signs of RV performance in COVID-19 ARDS.</p>\",\"PeriodicalId\":36911,\"journal\":{\"name\":\"Ultrasound Journal\",\"volume\":\"16 1\",\"pages\":\"26\"},\"PeriodicalIF\":3.6000,\"publicationDate\":\"2024-05-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11076422/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Ultrasound Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s13089-024-00366-5\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ultrasound Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13089-024-00366-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
Echocardiographic assessment of right ventricular performance in COVID-19 related acute respiratory distress syndrome: the importance of systo-diastolic interaction.
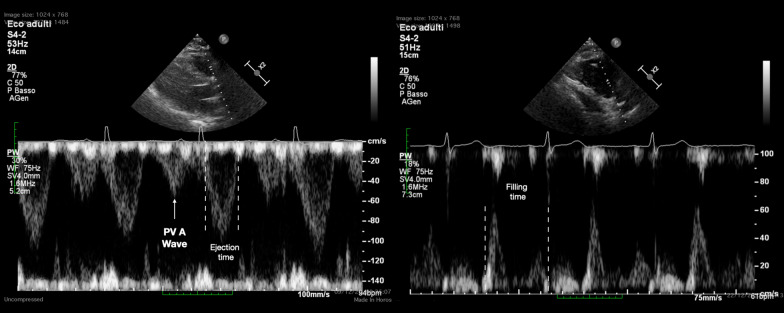
Background: The cardiac manifestations of COVID-19 have been described in patients with acute respiratory distress syndrome (ARDS) admitted to intensive care unit (ICU). The presence and impact of right ventricular (RV) diastolic function and performance has not been studied in this population yet. We describe the prevalence of RV diastolic dysfunction, assessed by the pulmonary valve pre-ejection A wave (PV A wave), and the RV systo-diastolic interaction, using the RV total isovolumic time (t-IVT), in COVID-19 ARDS.
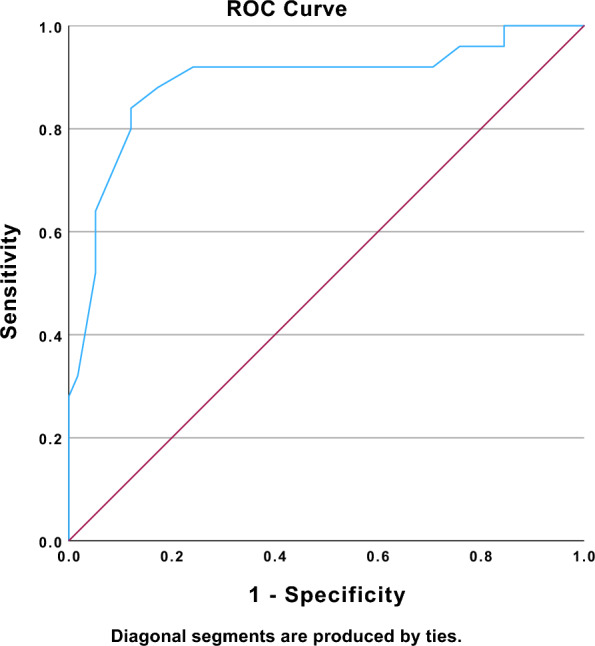
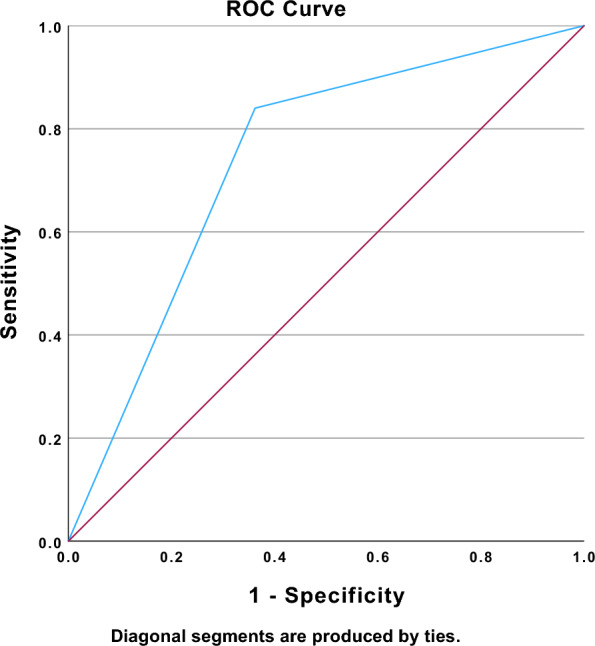
Results: Prospective observational study enrolling patients with moderate to severe COVID-19 ARDS admitted to ICU who underwent a transthoracic echocardiogram within 24 h of ICU admission and at least a second one during the ICU stay. Respiratory, hemodynamic and biochemistry parameters were collected. 163 patients (age 61.0 ± 9.3 years, 72% males) were enrolled. 36 patients (22.1%) had RV dysfunction, 45 (27.1%) LV systolic dysfunction. 73 patients (44.7%) had PV A wave. The RV t-IVT correlated with TAPSE at ICU admission (p < 0.002; r - 0.61), presence of PV A wave (p < 0.001; r 0.78), peak inspiratory pressure (PIP) (p < 0.001; r 0.42), PEEP (p < 0.001; r 0.68), dynamic driving pressure (DDP) (p < 0.001; r 0.58), and PaO2/FiO2 ratio (p < 0.01; r - 0.35). The presence of PV A wave was associated with higher PIP (p < 0.001; r 0.45), higher PEEP (p < 0.001; r 0.56), higher DDP (p < 0.01, r 0.51), and lower PaO2/FiO2 ratio (p < 0.001; r - 0.49).
Conclusions: RV t-IVT and the presence of PV A wave are non-invasive means to describe a significant RV diastolic dysfunction and may be consider descriptive signs of RV performance in COVID-19 ARDS.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
