{"title":"WEO 简讯:诀窍和技巧:炎症性肠病 (IBD) 狭窄处的评估和内镜扩张。","authors":"","doi":"10.1111/den.14902","DOIUrl":null,"url":null,"abstract":"<p>Gursimran S. Kochhar, MD, is a gastroenterologist, Division Chief of the Department of Gastroenterology and Hepatology, at Allegheny Health Network, Pittsburgh, Pennsylvania. He specializes in interventional inflammatory bowel disease (IBD) and advanced therapeutic procedures.</p><p>Dr. Kochhar completed his training in internal medicine at Cleveland Clinic Foundation, Cleveland, Ohio, where he subsequently received training in nutrition and finished a gastroenterology and hepatology fellowship focused on training in IBD. Dr. Kochhar then completed his advanced endoscopy fellowship at Mayo Clinic, Jacksonville, Florida.</p><p>Dr. Kochhar has been at the forefront of managing IBD and its complications with various advanced endoscopic procedures. His innovative research on the endoscopic management of IBD has been successfully published in leading gastroenterology journals, including Gastroenterology, Clinical Gastroenterology and Hepatology, and Gastrointestinal Endoscopy. He has more than 120 publications, including peer-reviewed articles and book chapters. He serves on the Editorial Board of the journal Inflammatory Bowel Diseases. His current research focuses on endoscopic management of IBD complications, artificial intelligence in health care, and newer endoscopic innovations.</p><p>Stricture formation is a common complication in Crohn's disease (CD) patients, resulting from the underlying disease process, surgical anastomosis, or strictureplasty. The true incidence of stricturing disease is hard to assess. However, some studies suggest the prevalence of strictures is up to 25% in patients with CD, and over 50% of patients with CD will need at least one surgery in their lifetime.</p><p>Endoscopic balloon dilation (EBD), first described by Dr. G.M. Heller in 1988 in a patient with CD,1 is a very important tool in our toolbox to manage strictures in such patients. EBD, if done well, can be very effective in mitigating or delaying surgeries in patients with CD (Fig. 1).</p><p>Endoscopic assessment of strictures is challenging, especially if they are impassable. Hence, we rely heavily on preprocedural imaging. Both computed tomography enterography (CTE) and magnetic resonance enterography (MRE) with contrast are acceptable preprocedural imaging techniques. These give us an idea of the length, number, severity, type of stricture (inflammatory versus fibrotic), presence of prestenotic dilation, and any associated fistula or abscess. All these details help us plan the procedure. Strictures longer than 5–7 cm or with significant prestenotic dilation (>5 cm in the small bowel) tend to be less responsive to EBD treatment. Avoid EBD in patients with an associated fistula or abscess. If there is a lot of inflammation on imaging, optimize medical therapy before performing an EBD.</p><p>Although there are not many scenarios where EBD is contraindicated, I recommend not performing it if there is an associated abscess or fistula with the stricture, as this may worsen the situation. Avoid EBD in patients with deep ulcerations, as these can easily cause perforation. For strictures longer than 5–6 cm, EBD may still be performed, but inform the patient of the limited success of endotherapy in such cases. EBD, in these cases of longer strictures, may serve as a bridge to surgery.</p><p>There are no clear guidelines on dilating asymptomatic strictures, making it a controversial issue. In my practice, I obtain preprocedural consent for EBD from patients with IBD. I dilate strictures even if patients are not symptomatic for several reasons. First, symptom correlation with stricture-related disease activity may not always align in CD patients; a significant stricture may present with minimal symptoms. EBD could help defer or prevent the development of symptomatic strictures. Additionally, incidentally identified strictures can impact the severity of future disease courses in IBD patients, including the development of partial small-bowel obstruction, fistula formation, and abscess formation.</p><p>EBD is a safe and efficacious endoscopic option for managing primary and anastomotic strictures. It aims to relieve obstructive symptoms and delay or avoid surgery. Patient selection and procedural planning are important to ensure this technique's success for our patients' benefit.</p>","PeriodicalId":159,"journal":{"name":"Digestive Endoscopy","volume":"36 8","pages":"961-964"},"PeriodicalIF":4.7000,"publicationDate":"2024-08-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14902","citationCount":"0","resultStr":"{\"title\":\"WEO Newsletter: Tips and tricks: Assessment and endoscopic dilation of strictures in inflammatory bowel disease (IBD)\",\"authors\":\"\",\"doi\":\"10.1111/den.14902\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Gursimran S. Kochhar, MD, is a gastroenterologist, Division Chief of the Department of Gastroenterology and Hepatology, at Allegheny Health Network, Pittsburgh, Pennsylvania. He specializes in interventional inflammatory bowel disease (IBD) and advanced therapeutic procedures.</p><p>Dr. Kochhar completed his training in internal medicine at Cleveland Clinic Foundation, Cleveland, Ohio, where he subsequently received training in nutrition and finished a gastroenterology and hepatology fellowship focused on training in IBD. Dr. Kochhar then completed his advanced endoscopy fellowship at Mayo Clinic, Jacksonville, Florida.</p><p>Dr. Kochhar has been at the forefront of managing IBD and its complications with various advanced endoscopic procedures. His innovative research on the endoscopic management of IBD has been successfully published in leading gastroenterology journals, including Gastroenterology, Clinical Gastroenterology and Hepatology, and Gastrointestinal Endoscopy. He has more than 120 publications, including peer-reviewed articles and book chapters. He serves on the Editorial Board of the journal Inflammatory Bowel Diseases. His current research focuses on endoscopic management of IBD complications, artificial intelligence in health care, and newer endoscopic innovations.</p><p>Stricture formation is a common complication in Crohn's disease (CD) patients, resulting from the underlying disease process, surgical anastomosis, or strictureplasty. The true incidence of stricturing disease is hard to assess. However, some studies suggest the prevalence of strictures is up to 25% in patients with CD, and over 50% of patients with CD will need at least one surgery in their lifetime.</p><p>Endoscopic balloon dilation (EBD), first described by Dr. G.M. Heller in 1988 in a patient with CD,1 is a very important tool in our toolbox to manage strictures in such patients. EBD, if done well, can be very effective in mitigating or delaying surgeries in patients with CD (Fig. 1).</p><p>Endoscopic assessment of strictures is challenging, especially if they are impassable. Hence, we rely heavily on preprocedural imaging. Both computed tomography enterography (CTE) and magnetic resonance enterography (MRE) with contrast are acceptable preprocedural imaging techniques. These give us an idea of the length, number, severity, type of stricture (inflammatory versus fibrotic), presence of prestenotic dilation, and any associated fistula or abscess. All these details help us plan the procedure. Strictures longer than 5–7 cm or with significant prestenotic dilation (>5 cm in the small bowel) tend to be less responsive to EBD treatment. Avoid EBD in patients with an associated fistula or abscess. If there is a lot of inflammation on imaging, optimize medical therapy before performing an EBD.</p><p>Although there are not many scenarios where EBD is contraindicated, I recommend not performing it if there is an associated abscess or fistula with the stricture, as this may worsen the situation. Avoid EBD in patients with deep ulcerations, as these can easily cause perforation. For strictures longer than 5–6 cm, EBD may still be performed, but inform the patient of the limited success of endotherapy in such cases. EBD, in these cases of longer strictures, may serve as a bridge to surgery.</p><p>There are no clear guidelines on dilating asymptomatic strictures, making it a controversial issue. In my practice, I obtain preprocedural consent for EBD from patients with IBD. I dilate strictures even if patients are not symptomatic for several reasons. First, symptom correlation with stricture-related disease activity may not always align in CD patients; a significant stricture may present with minimal symptoms. EBD could help defer or prevent the development of symptomatic strictures. Additionally, incidentally identified strictures can impact the severity of future disease courses in IBD patients, including the development of partial small-bowel obstruction, fistula formation, and abscess formation.</p><p>EBD is a safe and efficacious endoscopic option for managing primary and anastomotic strictures. It aims to relieve obstructive symptoms and delay or avoid surgery. Patient selection and procedural planning are important to ensure this technique's success for our patients' benefit.</p>\",\"PeriodicalId\":159,\"journal\":{\"name\":\"Digestive Endoscopy\",\"volume\":\"36 8\",\"pages\":\"961-964\"},\"PeriodicalIF\":4.7000,\"publicationDate\":\"2024-08-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/den.14902\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Digestive Endoscopy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/den.14902\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Digestive Endoscopy","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/den.14902","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
古尔西姆兰-科查尔(Gursimran S. Kochhar)医学博士是宾夕法尼亚州匹兹堡市阿勒格尼健康网络(Allegheny Health Network)的胃肠病学专家、胃肠病学和肝病学部主任。科查尔医生在俄亥俄州克利夫兰的克利夫兰诊所基金会完成了内科培训,随后在那里接受了营养学培训,并完成了胃肠病学和肝病学研究,重点是 IBD 培训。随后,科查尔医生在佛罗里达州杰克逊维尔市的梅奥诊所完成了高级内窥镜研究。科查尔医生一直走在利用各种高级内窥镜手术治疗肠道疾病及其并发症的前沿。他在内镜治疗 IBD 方面的创新研究成果已成功发表在《胃肠病学》、《临床胃肠病学与肝病学》和《胃肠内镜》等领先的胃肠病学期刊上。他发表了 120 多篇论文,包括同行评审文章和书籍章节。他还是《炎症性肠病》杂志编委会成员。他目前的研究重点是 IBD 并发症的内镜治疗、医疗保健中的人工智能以及较新的内镜创新技术。狭窄疾病的真正发病率很难评估。内镜下球囊扩张术(EBD)由 G.M. Heller 博士于 1988 年在一名 CD 患者身上首次描述1 ,是我们治疗此类患者狭窄的工具箱中非常重要的工具。如果操作得当,EBD 可以非常有效地减少或推迟 CD 患者的手术时间(图 1)。因此,我们在很大程度上依赖于术前成像。带对比剂的计算机断层扫描肠造影(CTE)和磁共振肠造影(MRE)都是可以接受的术前成像技术。通过这些检查,我们可以了解狭窄的长度、数量、严重程度、类型(炎症性还是纤维性)、是否存在狭窄前扩张以及是否存在相关的瘘管或脓肿。所有这些细节都有助于我们制定手术计划。狭窄长度超过 5-7 厘米或有明显狭窄前扩张(小肠为 5 厘米)的患者往往对 EBD 治疗反应较差。避免对伴有瘘管或脓肿的患者进行 EBD。虽然 EBD 的禁忌症并不多,但如果狭窄处伴有脓肿或瘘管,我建议不要进行 EBD,因为这可能会使情况恶化。避免对有深度溃疡的患者进行 EBD,因为这些溃疡很容易导致穿孔。对于长度超过 5-6 厘米的狭窄,仍然可以进行 EBD,但要告知患者在这种情况下内科治疗的成功率有限。对于这些较长的狭窄,EBD 可以作为手术的桥梁。对于无症状狭窄的扩张,目前还没有明确的指南,因此是一个有争议的问题。在我的临床实践中,我会在术前征得 IBD 患者对 EBD 的同意。出于几个原因,即使患者没有症状,我也会扩张狭窄。首先,在 CD 患者中,症状与狭窄相关疾病活动的相关性可能并不总是一致;严重的狭窄可能表现出极少的症状。EBD 有助于推迟或预防无症状狭窄的发生。此外,偶然发现的狭窄可能会影响 IBD 患者未来病程的严重程度,包括发展为部分小肠梗阻、瘘管形成和脓肿形成。其目的是缓解梗阻症状,推迟或避免手术。患者的选择和手术计划对于确保这项技术的成功并使患者受益非常重要。
WEO Newsletter: Tips and tricks: Assessment and endoscopic dilation of strictures in inflammatory bowel disease (IBD)
Gursimran S. Kochhar, MD, is a gastroenterologist, Division Chief of the Department of Gastroenterology and Hepatology, at Allegheny Health Network, Pittsburgh, Pennsylvania. He specializes in interventional inflammatory bowel disease (IBD) and advanced therapeutic procedures.
Dr. Kochhar completed his training in internal medicine at Cleveland Clinic Foundation, Cleveland, Ohio, where he subsequently received training in nutrition and finished a gastroenterology and hepatology fellowship focused on training in IBD. Dr. Kochhar then completed his advanced endoscopy fellowship at Mayo Clinic, Jacksonville, Florida.
Dr. Kochhar has been at the forefront of managing IBD and its complications with various advanced endoscopic procedures. His innovative research on the endoscopic management of IBD has been successfully published in leading gastroenterology journals, including Gastroenterology, Clinical Gastroenterology and Hepatology, and Gastrointestinal Endoscopy. He has more than 120 publications, including peer-reviewed articles and book chapters. He serves on the Editorial Board of the journal Inflammatory Bowel Diseases. His current research focuses on endoscopic management of IBD complications, artificial intelligence in health care, and newer endoscopic innovations.
Stricture formation is a common complication in Crohn's disease (CD) patients, resulting from the underlying disease process, surgical anastomosis, or strictureplasty. The true incidence of stricturing disease is hard to assess. However, some studies suggest the prevalence of strictures is up to 25% in patients with CD, and over 50% of patients with CD will need at least one surgery in their lifetime.
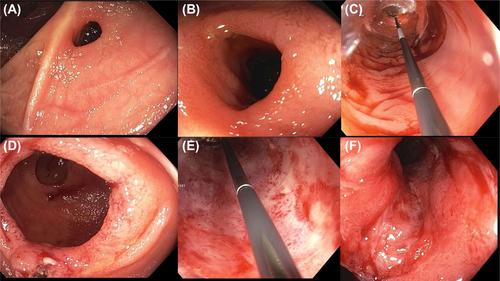
Endoscopic balloon dilation (EBD), first described by Dr. G.M. Heller in 1988 in a patient with CD,1 is a very important tool in our toolbox to manage strictures in such patients. EBD, if done well, can be very effective in mitigating or delaying surgeries in patients with CD (Fig. 1).
Endoscopic assessment of strictures is challenging, especially if they are impassable. Hence, we rely heavily on preprocedural imaging. Both computed tomography enterography (CTE) and magnetic resonance enterography (MRE) with contrast are acceptable preprocedural imaging techniques. These give us an idea of the length, number, severity, type of stricture (inflammatory versus fibrotic), presence of prestenotic dilation, and any associated fistula or abscess. All these details help us plan the procedure. Strictures longer than 5–7 cm or with significant prestenotic dilation (>5 cm in the small bowel) tend to be less responsive to EBD treatment. Avoid EBD in patients with an associated fistula or abscess. If there is a lot of inflammation on imaging, optimize medical therapy before performing an EBD.
Although there are not many scenarios where EBD is contraindicated, I recommend not performing it if there is an associated abscess or fistula with the stricture, as this may worsen the situation. Avoid EBD in patients with deep ulcerations, as these can easily cause perforation. For strictures longer than 5–6 cm, EBD may still be performed, but inform the patient of the limited success of endotherapy in such cases. EBD, in these cases of longer strictures, may serve as a bridge to surgery.
There are no clear guidelines on dilating asymptomatic strictures, making it a controversial issue. In my practice, I obtain preprocedural consent for EBD from patients with IBD. I dilate strictures even if patients are not symptomatic for several reasons. First, symptom correlation with stricture-related disease activity may not always align in CD patients; a significant stricture may present with minimal symptoms. EBD could help defer or prevent the development of symptomatic strictures. Additionally, incidentally identified strictures can impact the severity of future disease courses in IBD patients, including the development of partial small-bowel obstruction, fistula formation, and abscess formation.
EBD is a safe and efficacious endoscopic option for managing primary and anastomotic strictures. It aims to relieve obstructive symptoms and delay or avoid surgery. Patient selection and procedural planning are important to ensure this technique's success for our patients' benefit.
期刊介绍:
Digestive Endoscopy (DEN) is the official journal of the Japan Gastroenterological Endoscopy Society, the Asian Pacific Society for Digestive Endoscopy and the World Endoscopy Organization. Digestive Endoscopy serves as a medium for presenting original articles that offer significant contributions to knowledge in the broad field of endoscopy. The Journal also includes Reviews, Original Articles, How I Do It, Case Reports (only of exceptional interest and novelty are accepted), Letters, Techniques and Images, abstracts and news items that may be of interest to endoscopists.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
