Ellen M. Apperloo, Jose L. Gorriz, Maria Jose Soler, Secundino Cigarrán Guldris, Josep M. Cruzado, Maria Jesús Puchades, Marina López-Martínez, Femke Waanders, Gozewijn D. Laverman, Annemarie van der Aart-van der Beek, Klaas Hoogenberg, André P. van Beek, Jacobien Verhave, Sofia B. Ahmed, Roland E. Schmieder, Christoph Wanner, David Z. I. Cherney, Niels Jongs, Hiddo J. L. Heerspink
{"title":"塞马鲁肽治疗超重或肥胖且无糖尿病的慢性肾病患者:随机双盲安慰剂对照临床试验","authors":"Ellen M. Apperloo, Jose L. Gorriz, Maria Jose Soler, Secundino Cigarrán Guldris, Josep M. Cruzado, Maria Jesús Puchades, Marina López-Martínez, Femke Waanders, Gozewijn D. Laverman, Annemarie van der Aart-van der Beek, Klaas Hoogenberg, André P. van Beek, Jacobien Verhave, Sofia B. Ahmed, Roland E. Schmieder, Christoph Wanner, David Z. I. Cherney, Niels Jongs, Hiddo J. L. Heerspink","doi":"10.1038/s41591-024-03327-6","DOIUrl":null,"url":null,"abstract":"Semaglutide reduces albuminuria and the risk of kidney disease progression in patients with type 2 diabetes and chronic kidney disease (CKD). We conducted a randomized placebo-controlled double-blind clinical trial in adults with CKD (estimated glomerular filtration rate (eGFR) ≥25 ml min−1 1.73 m−2 and urine albumin-to-creatinine ratio (UACR) ≥30 and <3,500 mg g−1) and body mass index ≥27 kg m−2. Participants were randomized to semaglutide 2.4 mg per week or placebo. The primary endpoint was percentage change from baseline in UACR at week 24. Safety was monitored throughout. Overall, 125 participants were screened, of whom 101 were randomized to semaglutide (n = 51) or placebo (n = 50). Mean age was 55.8 (s.d. 12) years; 40 participants (39.6%) were female; median UACR was 251 mg g−1 (interquartile range 100, 584); mean eGFR was 65.0 (s.d. 25) ml min−1 1.73 m−2; and mean body mass index was 36.2 (s.d. 5.6) kg m−2. Chronic glomerulonephritis (n = 25) and hypertensive CKD (n = 27) were the most common CKD etiologies. Treatment for 24 weeks with semaglutide compared to placebo reduced UACR by −52.1% (95% confidence interval −65.5, −33.4; P < 0.0001). Gastrointestinal adverse events were more often reported with semaglutide (n = 30) than with placebo (n = 15). Semaglutide treatment for 24 weeks resulted in a clinically meaningful reduction in albuminuria in patients with overweight/obesity and non-diabetic CKD. ClinicalTrials.gov registration: NCT04889183 . In participants with obesity and chronic kidney disease without diabetes, once-weekly administration of semaglutide 2.4 mg led to a reduction in albuminuria, body weight and systolic blood pressure compared with placebo, with no changes to creatinine or cystatin-C estimated glomerular filtration rate or measured glomerular filtration rate during the 24-week follow-up period.","PeriodicalId":19037,"journal":{"name":"Nature Medicine","volume":"31 1","pages":"278-285"},"PeriodicalIF":50.0000,"publicationDate":"2024-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Semaglutide in patients with overweight or obesity and chronic kidney disease without diabetes: a randomized double-blind placebo-controlled clinical trial\",\"authors\":\"Ellen M. Apperloo, Jose L. Gorriz, Maria Jose Soler, Secundino Cigarrán Guldris, Josep M. Cruzado, Maria Jesús Puchades, Marina López-Martínez, Femke Waanders, Gozewijn D. Laverman, Annemarie van der Aart-van der Beek, Klaas Hoogenberg, André P. van Beek, Jacobien Verhave, Sofia B. Ahmed, Roland E. Schmieder, Christoph Wanner, David Z. I. Cherney, Niels Jongs, Hiddo J. L. Heerspink\",\"doi\":\"10.1038/s41591-024-03327-6\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"Semaglutide reduces albuminuria and the risk of kidney disease progression in patients with type 2 diabetes and chronic kidney disease (CKD). We conducted a randomized placebo-controlled double-blind clinical trial in adults with CKD (estimated glomerular filtration rate (eGFR) ≥25 ml min−1 1.73 m−2 and urine albumin-to-creatinine ratio (UACR) ≥30 and <3,500 mg g−1) and body mass index ≥27 kg m−2. Participants were randomized to semaglutide 2.4 mg per week or placebo. The primary endpoint was percentage change from baseline in UACR at week 24. Safety was monitored throughout. Overall, 125 participants were screened, of whom 101 were randomized to semaglutide (n = 51) or placebo (n = 50). Mean age was 55.8 (s.d. 12) years; 40 participants (39.6%) were female; median UACR was 251 mg g−1 (interquartile range 100, 584); mean eGFR was 65.0 (s.d. 25) ml min−1 1.73 m−2; and mean body mass index was 36.2 (s.d. 5.6) kg m−2. Chronic glomerulonephritis (n = 25) and hypertensive CKD (n = 27) were the most common CKD etiologies. Treatment for 24 weeks with semaglutide compared to placebo reduced UACR by −52.1% (95% confidence interval −65.5, −33.4; P < 0.0001). Gastrointestinal adverse events were more often reported with semaglutide (n = 30) than with placebo (n = 15). Semaglutide treatment for 24 weeks resulted in a clinically meaningful reduction in albuminuria in patients with overweight/obesity and non-diabetic CKD. ClinicalTrials.gov registration: NCT04889183 . In participants with obesity and chronic kidney disease without diabetes, once-weekly administration of semaglutide 2.4 mg led to a reduction in albuminuria, body weight and systolic blood pressure compared with placebo, with no changes to creatinine or cystatin-C estimated glomerular filtration rate or measured glomerular filtration rate during the 24-week follow-up period.\",\"PeriodicalId\":19037,\"journal\":{\"name\":\"Nature Medicine\",\"volume\":\"31 1\",\"pages\":\"278-285\"},\"PeriodicalIF\":50.0000,\"publicationDate\":\"2024-10-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nature Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://www.nature.com/articles/s41591-024-03327-6\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"BIOCHEMISTRY & MOLECULAR BIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nature Medicine","FirstCategoryId":"3","ListUrlMain":"https://www.nature.com/articles/s41591-024-03327-6","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
Semaglutide in patients with overweight or obesity and chronic kidney disease without diabetes: a randomized double-blind placebo-controlled clinical trial
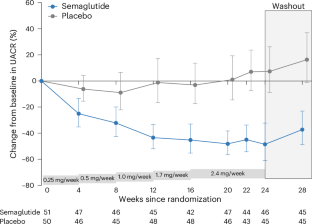
Semaglutide reduces albuminuria and the risk of kidney disease progression in patients with type 2 diabetes and chronic kidney disease (CKD). We conducted a randomized placebo-controlled double-blind clinical trial in adults with CKD (estimated glomerular filtration rate (eGFR) ≥25 ml min−1 1.73 m−2 and urine albumin-to-creatinine ratio (UACR) ≥30 and <3,500 mg g−1) and body mass index ≥27 kg m−2. Participants were randomized to semaglutide 2.4 mg per week or placebo. The primary endpoint was percentage change from baseline in UACR at week 24. Safety was monitored throughout. Overall, 125 participants were screened, of whom 101 were randomized to semaglutide (n = 51) or placebo (n = 50). Mean age was 55.8 (s.d. 12) years; 40 participants (39.6%) were female; median UACR was 251 mg g−1 (interquartile range 100, 584); mean eGFR was 65.0 (s.d. 25) ml min−1 1.73 m−2; and mean body mass index was 36.2 (s.d. 5.6) kg m−2. Chronic glomerulonephritis (n = 25) and hypertensive CKD (n = 27) were the most common CKD etiologies. Treatment for 24 weeks with semaglutide compared to placebo reduced UACR by −52.1% (95% confidence interval −65.5, −33.4; P < 0.0001). Gastrointestinal adverse events were more often reported with semaglutide (n = 30) than with placebo (n = 15). Semaglutide treatment for 24 weeks resulted in a clinically meaningful reduction in albuminuria in patients with overweight/obesity and non-diabetic CKD. ClinicalTrials.gov registration: NCT04889183 . In participants with obesity and chronic kidney disease without diabetes, once-weekly administration of semaglutide 2.4 mg led to a reduction in albuminuria, body weight and systolic blood pressure compared with placebo, with no changes to creatinine or cystatin-C estimated glomerular filtration rate or measured glomerular filtration rate during the 24-week follow-up period.
期刊介绍:
Nature Medicine is a monthly journal publishing original peer-reviewed research in all areas of medicine. The publication focuses on originality, timeliness, interdisciplinary interest, and the impact on improving human health. In addition to research articles, Nature Medicine also publishes commissioned content such as News, Reviews, and Perspectives. This content aims to provide context for the latest advances in translational and clinical research, reaching a wide audience of M.D. and Ph.D. readers. All editorial decisions for the journal are made by a team of full-time professional editors.
Nature Medicine consider all types of clinical research, including:
-Case-reports and small case series
-Clinical trials, whether phase 1, 2, 3 or 4
-Observational studies
-Meta-analyses
-Biomarker studies
-Public and global health studies
Nature Medicine is also committed to facilitating communication between translational and clinical researchers. As such, we consider “hybrid” studies with preclinical and translational findings reported alongside data from clinical studies.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
