{"title":"双相情感障碍门诊误诊分析。","authors":"Hui Shen, Li Zhang, Chuchen Xu, Jinling Zhu, Meijuan Chen, Yiru Fang","doi":"10.11919/j.issn.1002-0829.217080","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Bipolar disorder is a mental illness with a high misdiagnosis rate and commonly misdiagnosed as other mental disorders including depression, schizophrenia, anxiety disorders, obsessive-compulsive disorders, and personality disorders, resulting in the mistreatment of clinical symptoms and increasing of recurrent episodes.</p><p><strong>Aims: </strong>To understand the reasons for misdiagnosis of bipolar disorder in an outpatient setting in order to help clinicians more clearly identify the disease and avoid diagnostic errors.</p><p><strong>Methods: </strong>Data from an outpatient clinic included two groups: those with a confirmed diagnosis of bipolar disorder (CD group) and those who were misdiagnosed (i.e. those who did in fact have bipolar disorder but received a different diagnoses and those without bipolar disorder who received a bipolar diagnosis [MD group]). Information between these two groups was compared.</p><p><strong>Results: </strong>There were a total of 177 cases that met the inclusion criteria for this study. Among them, 136 cases (76.8%) were in the MD group and 41 cases (23.2%) were in the CD group. Patents with depression had the most cases of misdiagnosis (70.6%). The first episode of the patients in the MD group was more likely to be a depressive episode (χ<sup>2</sup>=5.206, <i>p</i>=0.023) and these patients had a greater number of depressive episodes during the course of the disease (<i>Z</i>=-2.268, <i>p</i>=0.023); the time from the onset of the disease to the first treatment was comparatively short (<i>Z</i>=-2.612, <i>p</i>=0.009) in the group with misdiagnosis; the time from the onset of disease to a confirmed diagnosis was longer (<i>Z</i>=-3.685, <i>p</i><0.001); the overall course of disease was longer (<i>Z</i>=-3.274, <i>p</i>=0.001); there were more inpatients for treatment (χ<sup>2</sup>=4.539, <i>p</i>=0.033); and hospitalization was more frequent (<i>Z</i>=-2.164, <i>p</i>=0.031). The group with misdiagnosis had more psychotic symptoms (χ<sup>2</sup>=11.74, <i>p</i>= 0.001); particularly when depression occurred (χ<sup>2</sup>=7.63, <i>p</i>= 0.006), and the incidence of comorbidity was higher (χ<sup>2</sup>=5.23, <i>p</i>=0.022). The HCL-32 rating was lower in the misdiagnosis group (<i>t</i>=-2.564, <i>p</i>=0.011). There were more patients diagnosed with bipolar and other related disorders in the misdiagnosis group than in the confirmed diagnosis group (11.0% v. 4.9%) and there were more patients in the MD group diagnosed with depressive episodes who had a recent episode (78.7% v. 65.9%).</p><p><strong>Conclusions: </strong>The rate of misdiagnosis of patients with bipolar receiving outpatient treatment was quite high and they often received a misdiagnosis of depression. In the misdiagnosis group the first episode tended to manifest as a depressive episode. In this group there were also a greater number of depressive episodes over the course of illness, accompanied by more psychotic symptoms and a higher incidence of comorbidity. Moreover, these patients apparently lacked insight into their own mania and hypomania symptoms, resulting in difficulties in early diagnosis, longer time needed to confirm the diagnosis, higher rate of hospitalization, and greater number of hospitalizations.</p>","PeriodicalId":21886,"journal":{"name":"上海精神医学","volume":"30 2","pages":"93-101"},"PeriodicalIF":0.0000,"publicationDate":"2018-04-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.11919/j.issn.1002-0829.217080","citationCount":"48","resultStr":"{\"title\":\"Analysis of Misdiagnosis of Bipolar Disorder in An Outpatient Setting.\",\"authors\":\"Hui Shen, Li Zhang, Chuchen Xu, Jinling Zhu, Meijuan Chen, Yiru Fang\",\"doi\":\"10.11919/j.issn.1002-0829.217080\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Bipolar disorder is a mental illness with a high misdiagnosis rate and commonly misdiagnosed as other mental disorders including depression, schizophrenia, anxiety disorders, obsessive-compulsive disorders, and personality disorders, resulting in the mistreatment of clinical symptoms and increasing of recurrent episodes.</p><p><strong>Aims: </strong>To understand the reasons for misdiagnosis of bipolar disorder in an outpatient setting in order to help clinicians more clearly identify the disease and avoid diagnostic errors.</p><p><strong>Methods: </strong>Data from an outpatient clinic included two groups: those with a confirmed diagnosis of bipolar disorder (CD group) and those who were misdiagnosed (i.e. those who did in fact have bipolar disorder but received a different diagnoses and those without bipolar disorder who received a bipolar diagnosis [MD group]). Information between these two groups was compared.</p><p><strong>Results: </strong>There were a total of 177 cases that met the inclusion criteria for this study. Among them, 136 cases (76.8%) were in the MD group and 41 cases (23.2%) were in the CD group. Patents with depression had the most cases of misdiagnosis (70.6%). The first episode of the patients in the MD group was more likely to be a depressive episode (χ<sup>2</sup>=5.206, <i>p</i>=0.023) and these patients had a greater number of depressive episodes during the course of the disease (<i>Z</i>=-2.268, <i>p</i>=0.023); the time from the onset of the disease to the first treatment was comparatively short (<i>Z</i>=-2.612, <i>p</i>=0.009) in the group with misdiagnosis; the time from the onset of disease to a confirmed diagnosis was longer (<i>Z</i>=-3.685, <i>p</i><0.001); the overall course of disease was longer (<i>Z</i>=-3.274, <i>p</i>=0.001); there were more inpatients for treatment (χ<sup>2</sup>=4.539, <i>p</i>=0.033); and hospitalization was more frequent (<i>Z</i>=-2.164, <i>p</i>=0.031). The group with misdiagnosis had more psychotic symptoms (χ<sup>2</sup>=11.74, <i>p</i>= 0.001); particularly when depression occurred (χ<sup>2</sup>=7.63, <i>p</i>= 0.006), and the incidence of comorbidity was higher (χ<sup>2</sup>=5.23, <i>p</i>=0.022). The HCL-32 rating was lower in the misdiagnosis group (<i>t</i>=-2.564, <i>p</i>=0.011). There were more patients diagnosed with bipolar and other related disorders in the misdiagnosis group than in the confirmed diagnosis group (11.0% v. 4.9%) and there were more patients in the MD group diagnosed with depressive episodes who had a recent episode (78.7% v. 65.9%).</p><p><strong>Conclusions: </strong>The rate of misdiagnosis of patients with bipolar receiving outpatient treatment was quite high and they often received a misdiagnosis of depression. In the misdiagnosis group the first episode tended to manifest as a depressive episode. In this group there were also a greater number of depressive episodes over the course of illness, accompanied by more psychotic symptoms and a higher incidence of comorbidity. Moreover, these patients apparently lacked insight into their own mania and hypomania symptoms, resulting in difficulties in early diagnosis, longer time needed to confirm the diagnosis, higher rate of hospitalization, and greater number of hospitalizations.</p>\",\"PeriodicalId\":21886,\"journal\":{\"name\":\"上海精神医学\",\"volume\":\"30 2\",\"pages\":\"93-101\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2018-04-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.11919/j.issn.1002-0829.217080\",\"citationCount\":\"48\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"上海精神医学\",\"FirstCategoryId\":\"95\",\"ListUrlMain\":\"https://doi.org/10.11919/j.issn.1002-0829.217080\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"上海精神医学","FirstCategoryId":"95","ListUrlMain":"https://doi.org/10.11919/j.issn.1002-0829.217080","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Analysis of Misdiagnosis of Bipolar Disorder in An Outpatient Setting.
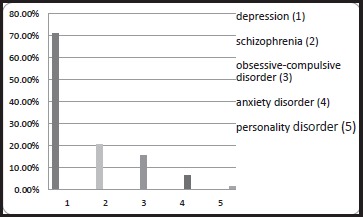
Background: Bipolar disorder is a mental illness with a high misdiagnosis rate and commonly misdiagnosed as other mental disorders including depression, schizophrenia, anxiety disorders, obsessive-compulsive disorders, and personality disorders, resulting in the mistreatment of clinical symptoms and increasing of recurrent episodes.
Aims: To understand the reasons for misdiagnosis of bipolar disorder in an outpatient setting in order to help clinicians more clearly identify the disease and avoid diagnostic errors.
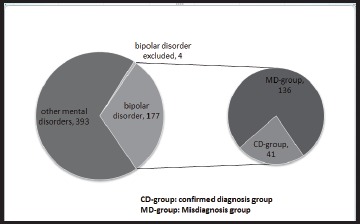
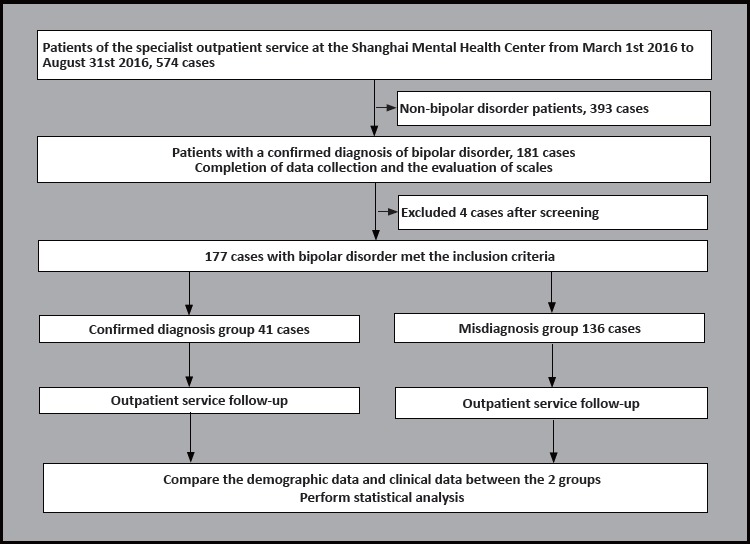
Methods: Data from an outpatient clinic included two groups: those with a confirmed diagnosis of bipolar disorder (CD group) and those who were misdiagnosed (i.e. those who did in fact have bipolar disorder but received a different diagnoses and those without bipolar disorder who received a bipolar diagnosis [MD group]). Information between these two groups was compared.
Results: There were a total of 177 cases that met the inclusion criteria for this study. Among them, 136 cases (76.8%) were in the MD group and 41 cases (23.2%) were in the CD group. Patents with depression had the most cases of misdiagnosis (70.6%). The first episode of the patients in the MD group was more likely to be a depressive episode (χ2=5.206, p=0.023) and these patients had a greater number of depressive episodes during the course of the disease (Z=-2.268, p=0.023); the time from the onset of the disease to the first treatment was comparatively short (Z=-2.612, p=0.009) in the group with misdiagnosis; the time from the onset of disease to a confirmed diagnosis was longer (Z=-3.685, p<0.001); the overall course of disease was longer (Z=-3.274, p=0.001); there were more inpatients for treatment (χ2=4.539, p=0.033); and hospitalization was more frequent (Z=-2.164, p=0.031). The group with misdiagnosis had more psychotic symptoms (χ2=11.74, p= 0.001); particularly when depression occurred (χ2=7.63, p= 0.006), and the incidence of comorbidity was higher (χ2=5.23, p=0.022). The HCL-32 rating was lower in the misdiagnosis group (t=-2.564, p=0.011). There were more patients diagnosed with bipolar and other related disorders in the misdiagnosis group than in the confirmed diagnosis group (11.0% v. 4.9%) and there were more patients in the MD group diagnosed with depressive episodes who had a recent episode (78.7% v. 65.9%).
Conclusions: The rate of misdiagnosis of patients with bipolar receiving outpatient treatment was quite high and they often received a misdiagnosis of depression. In the misdiagnosis group the first episode tended to manifest as a depressive episode. In this group there were also a greater number of depressive episodes over the course of illness, accompanied by more psychotic symptoms and a higher incidence of comorbidity. Moreover, these patients apparently lacked insight into their own mania and hypomania symptoms, resulting in difficulties in early diagnosis, longer time needed to confirm the diagnosis, higher rate of hospitalization, and greater number of hospitalizations.
期刊介绍:
Shanghai archives of psychiatry (bimonthly) was founded in 1959 and is sponsored by Shanghai Mental Health Center. The journal is aimed at mental health workers across the country, including psychiatrists and nurses, clinical psychologists, social workers, and people who are committed to the cause of mental health. It focuses on reporting clinical research results and practical experience in the field of psychiatry, and introduces the latest knowledge in psychiatry and related fields. The columns include monographs, case reports, clinical case discussions, reviews, mental health and law, and debates and discussions.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
