Carlos A Munoz-Zuluaga, Armando Sardi, Michelle Sittig, Vadim Gushchin, Mary C King, Carol Nieroda, Felipe Lopez-Ramirez, Teresa P Diaz-Montes
{"title":"IV期上皮性卵巢癌患者接受新辅助化疗后细胞减少手术和腹腔热化疗(CRS/HIPEC)的关键分析。","authors":"Carlos A Munoz-Zuluaga, Armando Sardi, Michelle Sittig, Vadim Gushchin, Mary C King, Carol Nieroda, Felipe Lopez-Ramirez, Teresa P Diaz-Montes","doi":"10.1155/2020/1467403","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (CRS/HIPEC) after neoadjuvant chemotherapy (NACT) showed promise as initial treatment for stage IIIC (SIII) epithelial ovarian cancer (EOC); however, stage IV (SIV) outcomes are rarely reported. We assessed our experience and outcomes treating newly diagnosed SIV EOC with NACT plus CRS/HIPEC compared to SIII patients.</p><p><strong>Methods: </strong>Advanced EOC from 2015-2018 managed with NACT (carboplatin/paclitaxel) due to unresectable disease or poor performance status followed by interval CRS/HIPEC were reviewed. Perioperative factors were assessed. Overall survival (OS) and progression-free survival (PFS) were analyzed by stage.</p><p><strong>Results: </strong>Twenty-seven FIGO stage IIIC (<i>n</i> = 12) and IV (<i>n</i> = 15) patients were reviewed. Median NACT cycles were 3 and 4, respectively. Post-NACT omental caking, ascites, and pleural effusions decreased/resolved in 91%, 91%, and 100% of SIII and 85%, 92%, and 71% of SIV. SIII/SIV median PCI was 21 and 20 obtaining 92% and 100% complete cytoreduction (≤0.25 cm), respectively. Median organ resections were 6 and 7, respectively. Grade III/IV surgical complications were 0% SIII and 23% SIV, without hospital mortality. Median time to adjuvant chemotherapy was 53 and 74 days, respectively (<i>p</i>=0.007). SIII OS at 1 and 2 years was 100% and 83% and 87% and 76% in SIV (<i>p</i>=0.269). SIII 1-year PFS was 54%; median PFS: 12 months. SIV 1- and 2- year PFS was 47% and 23%; median PFS: 12 months (<i>p</i>=0.944).</p><p><strong>Conclusion: </strong>Outcomes in select initially diagnosed and unresectable SIV EOC are similar to SIII after NACT plus CRS/HIPEC. SIV EOC may benefit from CRS/HIPEC, and further studies should explore this treatment approach.</p>","PeriodicalId":45960,"journal":{"name":"International Journal of Surgical Oncology","volume":"2020 ","pages":"1467403"},"PeriodicalIF":1.6000,"publicationDate":"2020-12-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1155/2020/1467403","citationCount":"2","resultStr":"{\"title\":\"Critical Analysis of Stage IV Epithelial Ovarian Cancer Patients after Treatment with Neoadjuvant Chemotherapy followed by Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy (CRS/HIPEC).\",\"authors\":\"Carlos A Munoz-Zuluaga, Armando Sardi, Michelle Sittig, Vadim Gushchin, Mary C King, Carol Nieroda, Felipe Lopez-Ramirez, Teresa P Diaz-Montes\",\"doi\":\"10.1155/2020/1467403\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (CRS/HIPEC) after neoadjuvant chemotherapy (NACT) showed promise as initial treatment for stage IIIC (SIII) epithelial ovarian cancer (EOC); however, stage IV (SIV) outcomes are rarely reported. We assessed our experience and outcomes treating newly diagnosed SIV EOC with NACT plus CRS/HIPEC compared to SIII patients.</p><p><strong>Methods: </strong>Advanced EOC from 2015-2018 managed with NACT (carboplatin/paclitaxel) due to unresectable disease or poor performance status followed by interval CRS/HIPEC were reviewed. Perioperative factors were assessed. Overall survival (OS) and progression-free survival (PFS) were analyzed by stage.</p><p><strong>Results: </strong>Twenty-seven FIGO stage IIIC (<i>n</i> = 12) and IV (<i>n</i> = 15) patients were reviewed. Median NACT cycles were 3 and 4, respectively. Post-NACT omental caking, ascites, and pleural effusions decreased/resolved in 91%, 91%, and 100% of SIII and 85%, 92%, and 71% of SIV. SIII/SIV median PCI was 21 and 20 obtaining 92% and 100% complete cytoreduction (≤0.25 cm), respectively. Median organ resections were 6 and 7, respectively. Grade III/IV surgical complications were 0% SIII and 23% SIV, without hospital mortality. Median time to adjuvant chemotherapy was 53 and 74 days, respectively (<i>p</i>=0.007). SIII OS at 1 and 2 years was 100% and 83% and 87% and 76% in SIV (<i>p</i>=0.269). SIII 1-year PFS was 54%; median PFS: 12 months. SIV 1- and 2- year PFS was 47% and 23%; median PFS: 12 months (<i>p</i>=0.944).</p><p><strong>Conclusion: </strong>Outcomes in select initially diagnosed and unresectable SIV EOC are similar to SIII after NACT plus CRS/HIPEC. SIV EOC may benefit from CRS/HIPEC, and further studies should explore this treatment approach.</p>\",\"PeriodicalId\":45960,\"journal\":{\"name\":\"International Journal of Surgical Oncology\",\"volume\":\"2020 \",\"pages\":\"1467403\"},\"PeriodicalIF\":1.6000,\"publicationDate\":\"2020-12-16\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://sci-hub-pdf.com/10.1155/2020/1467403\",\"citationCount\":\"2\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International Journal of Surgical Oncology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1155/2020/1467403\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2020/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Surgical Oncology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2020/1467403","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ONCOLOGY","Score":null,"Total":0}
Critical Analysis of Stage IV Epithelial Ovarian Cancer Patients after Treatment with Neoadjuvant Chemotherapy followed by Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy (CRS/HIPEC).
Background: Cytoreductive surgery and hyperthermic intraperitoneal chemotherapy (CRS/HIPEC) after neoadjuvant chemotherapy (NACT) showed promise as initial treatment for stage IIIC (SIII) epithelial ovarian cancer (EOC); however, stage IV (SIV) outcomes are rarely reported. We assessed our experience and outcomes treating newly diagnosed SIV EOC with NACT plus CRS/HIPEC compared to SIII patients.
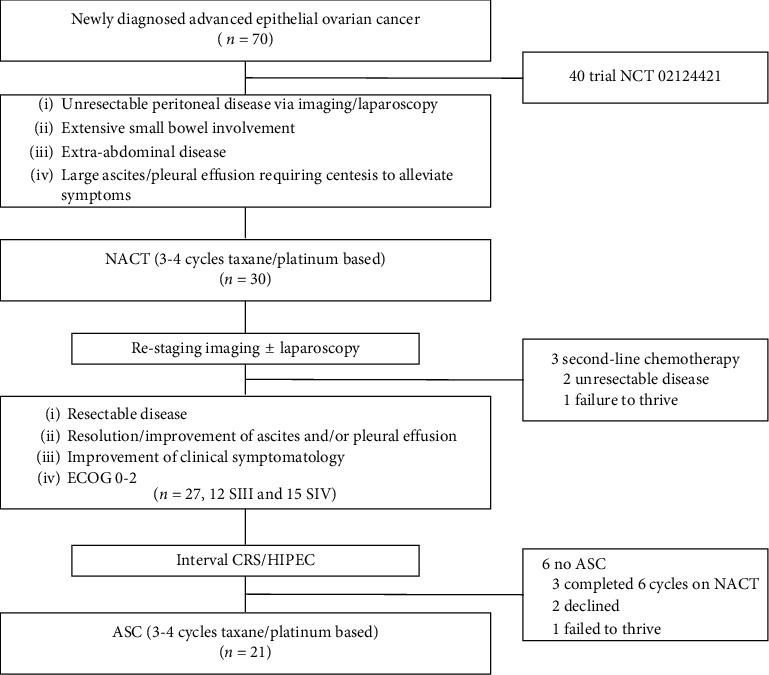
Methods: Advanced EOC from 2015-2018 managed with NACT (carboplatin/paclitaxel) due to unresectable disease or poor performance status followed by interval CRS/HIPEC were reviewed. Perioperative factors were assessed. Overall survival (OS) and progression-free survival (PFS) were analyzed by stage.
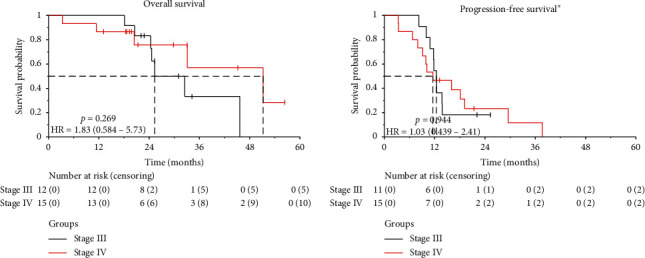
Results: Twenty-seven FIGO stage IIIC (n = 12) and IV (n = 15) patients were reviewed. Median NACT cycles were 3 and 4, respectively. Post-NACT omental caking, ascites, and pleural effusions decreased/resolved in 91%, 91%, and 100% of SIII and 85%, 92%, and 71% of SIV. SIII/SIV median PCI was 21 and 20 obtaining 92% and 100% complete cytoreduction (≤0.25 cm), respectively. Median organ resections were 6 and 7, respectively. Grade III/IV surgical complications were 0% SIII and 23% SIV, without hospital mortality. Median time to adjuvant chemotherapy was 53 and 74 days, respectively (p=0.007). SIII OS at 1 and 2 years was 100% and 83% and 87% and 76% in SIV (p=0.269). SIII 1-year PFS was 54%; median PFS: 12 months. SIV 1- and 2- year PFS was 47% and 23%; median PFS: 12 months (p=0.944).
Conclusion: Outcomes in select initially diagnosed and unresectable SIV EOC are similar to SIII after NACT plus CRS/HIPEC. SIV EOC may benefit from CRS/HIPEC, and further studies should explore this treatment approach.
期刊介绍:
International Journal of Surgical Oncology is a peer-reviewed, Open Access journal that publishes original research articles, review articles, and clinical studies in all areas of surgical oncology.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
