{"title":"Evaluation of pediatric gunshot wounds and emergency department dynamics in high-volume incidents.","authors":"Gulbin Aydogdu Umac, Remzi Cetinkaya, Mehmet Ozel, Habip Balsak, Sarper Yilmaz","doi":"10.14744/tjtes.2025.35961","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Pediatric gunshot injuries present significant challenges to emergency care, highlighting the need for precise strategies in the management of high-volume incidents. This study aims to assess pediatric gunshot injuries presenting to the emergency department in clusters and their outcomes, contributing to the development of a more detailed high-volume incidents classification based on patient numbers.</p><p><strong>Methods: </strong>A retrospective analysis was conducted at a level-one trauma center, focusing on pediatric gunshot admissions. Patients were segmented by admission type: single versus multiple simultaneous admissions from the same incident. Further analysis distinguished between incidents involving three or more victims and those with fewer victims to assess the impact on emergency care outcomes.</p><p><strong>Results: </strong>This study included 182 pediatric patients with gunshot injuries, with a median age of 16 years (IQR 13.75-17). Patients were analyzed using two grouping methods: the first divided patients into single admissions (n=103, 56.6%) and multi-victim presentations (n=79, 43.4%). In this comparison, multi-victim presentations had a lower rate of blood transfusions (RR: 0.58, 95% CI: 0.35-0.95) but similar mortality rates (RR: 0.88, 95% CI: 0.31-2.44). The second grouping method classified incidents with three or more victims (n=35, 19.2%) versus fewer victims (n=147, 80.8%). This analysis showed that incidents with three or more victims had a higher mortality rate (RR: 2.81, 95% CI: 1.08-7.31). The average ED stay was shorter for multi-victim presentations (54.1+-22.5 minutes) compared to solo presentations (65.2+-48.8 minutes).</p><p><strong>Conclusion: </strong>Findings indicate that pediatric gunshot incidents with three or more simultaneous victims, regardless of triage category, significantly affect mortality and ED stay lengths in a center with a single trauma team. This highlights the necessity of defining MCIs based on such patient volumes to optimize emergency care responses and improve outcomes. Establishing objective, outcome-focused criteria for high-volume incidents classification is crucial for enhancing patient care and resource allocation in these critical situations.</p>","PeriodicalId":94263,"journal":{"name":"Ulusal travma ve acil cerrahi dergisi = Turkish journal of trauma & emergency surgery : TJTES","volume":"31 2","pages":"167-177"},"PeriodicalIF":1.0000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11843418/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ulusal travma ve acil cerrahi dergisi = Turkish journal of trauma & emergency surgery : TJTES","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14744/tjtes.2025.35961","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Pediatric gunshot injuries present significant challenges to emergency care, highlighting the need for precise strategies in the management of high-volume incidents. This study aims to assess pediatric gunshot injuries presenting to the emergency department in clusters and their outcomes, contributing to the development of a more detailed high-volume incidents classification based on patient numbers.
Methods: A retrospective analysis was conducted at a level-one trauma center, focusing on pediatric gunshot admissions. Patients were segmented by admission type: single versus multiple simultaneous admissions from the same incident. Further analysis distinguished between incidents involving three or more victims and those with fewer victims to assess the impact on emergency care outcomes.
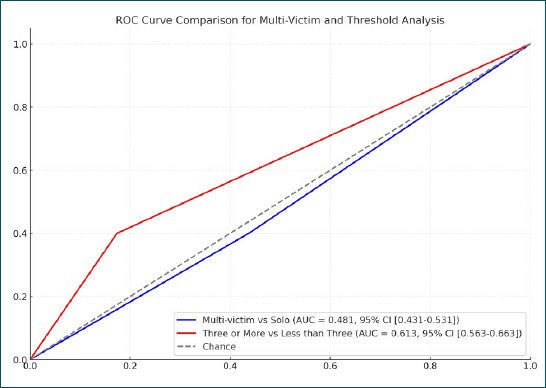
Results: This study included 182 pediatric patients with gunshot injuries, with a median age of 16 years (IQR 13.75-17). Patients were analyzed using two grouping methods: the first divided patients into single admissions (n=103, 56.6%) and multi-victim presentations (n=79, 43.4%). In this comparison, multi-victim presentations had a lower rate of blood transfusions (RR: 0.58, 95% CI: 0.35-0.95) but similar mortality rates (RR: 0.88, 95% CI: 0.31-2.44). The second grouping method classified incidents with three or more victims (n=35, 19.2%) versus fewer victims (n=147, 80.8%). This analysis showed that incidents with three or more victims had a higher mortality rate (RR: 2.81, 95% CI: 1.08-7.31). The average ED stay was shorter for multi-victim presentations (54.1+-22.5 minutes) compared to solo presentations (65.2+-48.8 minutes).
Conclusion: Findings indicate that pediatric gunshot incidents with three or more simultaneous victims, regardless of triage category, significantly affect mortality and ED stay lengths in a center with a single trauma team. This highlights the necessity of defining MCIs based on such patient volumes to optimize emergency care responses and improve outcomes. Establishing objective, outcome-focused criteria for high-volume incidents classification is crucial for enhancing patient care and resource allocation in these critical situations.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
